An interesting case of primary cutaneous actinomycosis
Published Web Location
https://doi.org/10.5070/D39x96h2pzMain Content
An interesting case of primary cutaneous actinomycosis
Debabrata Roy MS FRCS, Pankaj Gupta Roy MS FRCS, and PK Misra MS
Dermatology Online Journal 9 (5): 17
Department of Surgery, Sant Parmanand Hospital, New Delhi, India. dr_pankaj@hotmail.com
Abstract
Actinomycosis is an infection commonly seen in tropical countries. It is characterized by chronic and progressive suppurative inflammation, typically presenting on the neck, thorax, and abdomen. Primary cutaneous actinomycosis is a rare entity, and the diagnosis requires a high index of clinical suspicion. Anaerobic cultures may be negative despite repeated attempts. Microscopic examination reveals the diagnosis in the majority of cases, and treatment requires administration of parenteral or oral penicillin for at least 6 weeks. We report a case of cutaneous actinomycosis affecting the arm. This patient was treated with phenoxymethylpenicillin.
Introduction
Actinomycosis is a chronic and suppurative infection caused by an endogenous gram-positive bacterium, Actinomyces israelii. The usual sites of infection are the head and neck, thorax, and abdomen. Primary disease of the extremities is uncommon and has an association with trauma and bites. The main differential diagnosis is tuberculosis; the distinction can be made by the histopathology examination.
Case report
A 26-year-old woman presented in the outpatient clinic with a swelling on the outer aspect of her left upper arm. She had noticed a small painful nodule about a year previously. The nodule had become soft and subsided spontaneously after discharging pus. The lesion recurred after a short period and gradually increased in size. Areas of spontaneous breakdown drained clear fluid and pus. She had received three different antibiotics over the 1-year period, which yielded only a partial response or no response at all. She had no systemic symptoms.

|
|
| Figure 1 | Figure 2 |
|---|---|
| An indurated lesion with overlying papules, nodules, and sinuses on the left upper arm (fig. 1). | |
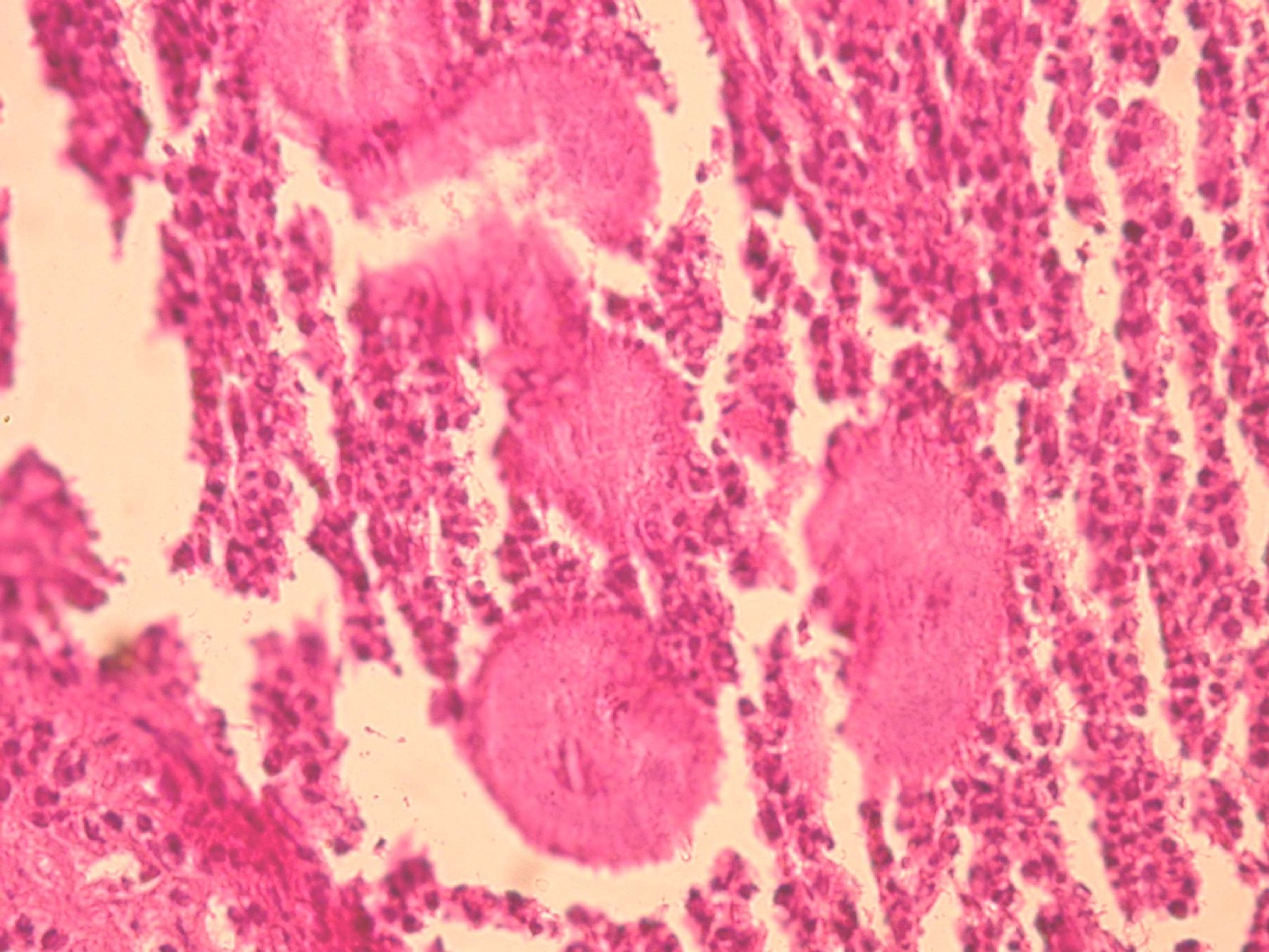
| Colonies of Actinomyces sp. surrounded by neutrophils (H&E stain, 40 magnification) (fig.2). | |
The clinical examination revealed a 10 × 12-cm firm, nontender swelling on the lateral aspect of left upper arm, fixed to the underlying muscles. The overlying skin was adherent, scarred in places, with papules and nodules; some were draining either clear or serosanguinous fluid (fig. 1). There was no palpable lymphadenopathy. The patient was given an initial clinical diagnosis of tuberculosis or actinomycosis. The routine hematological and biochemical tests were normal. X-rays of the arm did not show any evidence of osteomyelitis. The microbiological (aerobic and anaerobic) cultures showed no growth.
Fine-needle-aspiration cytology revealed nonspecific acute and chronic inflammation. The acid-fast-stained smear for Mycobacterium tuberculosis was negative. The microscopic examination of the skin biopsy revealed the presence of organisms resembling Actinomyces sp. surrounded by neutrophils in the dermis (fig. 2). The diagnosis of primary cutaneous actinomycosis was made, and the patient was treated successfully with oral penicillin.
Discussion
Actinomyces israelii is a normal inhabitant of the oral cavity. Infections are considered to be endogenous and the organism becomes pathogenic in the presence of devitalized tissues with reduced oxygen tension. Thus, actinomycosis may develop in the jaw and neck after an infection or dental surgery or in lung or gut when superimposed on an antecedent disorder that provides a favorable environment for its growth (e.g., lung abscess, ulcero-inflammatory disease of the gut). Grossly, it presents as intense suppuration with abscess and sinus formation discharging yellow sulphur granules. Histology is diagnostic, characteristically showing colonies (sulphur granules) formed by tangled mass of filaments surrounded by radiating, sometimes terminally clubbed, organisms [1].
Primary actinomycosis of the extremity [2, 3, 4] is rare because of the exclusively endogenous habitat of the etiologic organism. The majority of the cases reported have had a clear history of trauma, either a human bite or a perforating injury with contamination from outside [2]. Hematogenous spread has also been suggested in the literature [5]. In our patient's case, there was no history suggesting trauma, and so the exact pathogenesis remains unclear. The repeated attempts to culture the organism were unsuccessful, and the diagnosis was established by histopathology. The patient was treated successfully with oral penicillin over a period of 3 months.
Acknowledgment: I wish to thank Dr. V. M. Joglekar, Consultant Histopathologist, Furness General Hospital, Barrow-in-Furness, UK for his valuable help and guidance.
References
1. Lungs and upper respiratory tract. In: Kumar, Cotrans, Robbins, eds (1997) Basic Pathology. 6th edition WB Saunders, Philadelphia: 420.2. Reiner SL, Harrelson JM, Miller SE, Hill GB, Gallis HA. Primary actinomycosis of an extremity: a case report and review. Rev Infect Dis. 1987 May-Jun;9(3):581-9. PubMed
3. Sardana K, Mendiratta V, Sharma RC. A suspected case of primary cutaneous actinomycosis on the buttock. J Dermatol. 2001 May;28(5):276-8. PubMed
4. Wee SH, Chang SN, Shim JY, Chun SL, Park WH. A case of primary cutaneous actinomycosis. J Dermatol. 2000 Oct;27(10):651-4. PubMed
5. Butas CA, Read SE, Coleman RE, Abravoltch M. Disseminated actinomycosis. Can Med Assoc J. 1970 Nov 7;103(10):1069-71. No abstract available. PubMed
© 2003 Dermatology Online Journal