Bilateral facial pigmentation
Published Web Location
https://doi.org/10.5070/D39rt264z9Main Content
Bilateral facial pigmentation
Y Connie Chang MD, Nancy Anderson MD, Fred Soeprono MD JD
Dermatology Online Journal 13 (3): 16
Loma Linda University Medical Center, Loma Linda, CAAbstract
A 38-year-old man presented with a chief complaint of blue-speckled secretions on his cheeks, brought on by exertion. Based on the clinical features, a diagnosis of apocrine chromhidrosis was made. Histopathologic exam further supported this diagnosis. Possible treatment options for apocrine chromhidrosis are discussed.
Clinical Synopsis
A 38-year-old man presented with a 5-year history of subtle, dark blue secretions on bilateral malar cheeks. Pin-point pigmented specks would appear with exertion, most noticeably with exercise. The patient's other bodily secretions were normal in color. He denied any symptoms of arthropathy or back pain. His medical history was otherwise unremarkable, and he was not on any topical or oral medications.
 |
| Figure 1 |
|---|
Physical examination revealed a type-II skin with a subtle blue hue to bilateral superior malar cheeks. Upon moderate exertion (running in place), small blue-black beads of sweat appeared in a symmetric, diffuse pattern (Fig. 1). Urinary homogentisic acid levels and lumbar spinal x-rays were normal.
 | 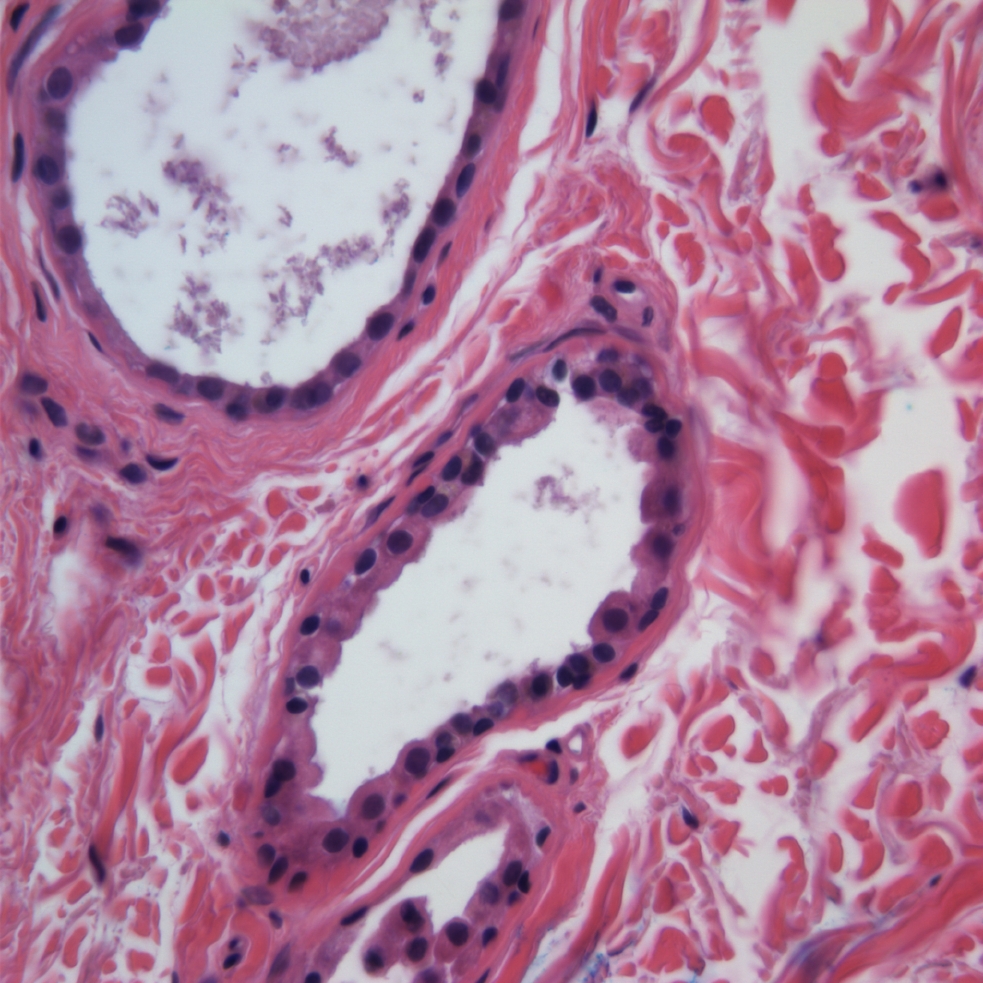 |
| Figure 2 | Figure 3 |
|---|
A 3-mm punch biopsy specimen was obtained (Figs. 2 and 3). Histopathologic examination revealed glandular structures exhibiting decapitation secretion, consistent with ectopic apocrine glands in the deep reticular dermis. Bluish cytoplasmic granules were observed in the apocrine epithelium lining. The diagnosis of facial apocrine chromhidrosis was made. Potential treatment options including 20 percent aluminum chloride hexahydrate solution (Drysol), capsaicin cream, and botulinum toxin-A were discussed with the patient. However, he deferred active treatment at this time.
Comment
Chromhidrosis is a rare idiopathic disorder of eccrine or apocrine sweat glands, characterized by yellow, blue, green, or black pigmented secretions. In most cases, chromhidrosis appears unrelated to diet, systemic, or metabolic abnormalities. Several etiologies for chromhidrosis exist. True eccrine chromhidrosis is associated with water-soluble pigments excreted by the eccrine glands. Pseudochromhidrosis is the result of colorless perspiration mixed with an external chromogen such as dyed clothing. Apocrine chromhidrosis results from a higher concentration of lipofuscin granules in the apocrine gland [1]. The majority of case reports in the literature have been confined to the malar cheeks [1, 2, 3, 4], but axillary and areolar chromhidrosis also have been reported [5, 6].
Chromhidrosis is a simple clinical diagnosis to make, but a more challenging one to treat. Topical treatment options include 20 percent aluminum chloride hexahydrate solution (Drysol), and capsaicin cream (a topical agent that depletes neurons of substance P, a transmitter in apocrine sweat production) [4]. Both are temporary measures of therapy with chromhidrosis returning with discontinuation of medication application. More recently, botulinum toxin type A (BTX-A), a chemodenervating agent FDA approved for the treatment of blepharospasm, strabismus, and glabellar rhytides, has been shown to be effective for facial chromhidrosis for up to 19 weeks post-treatment [3]. The BTX-A likely works through multiple mechanisms. It prevents the release of acetylcholine at the presynaptic motor neuromuscular plate, effectively blocking the parasympathetic stimulation necessary for sweat gland stimuli, and it has also been shown to inhibit substance-P release. In addition, the myoepithelium surrounding eccrine glands is susceptible to acetylcholine stimulation; inhibition of acetylcholine release at this level may help prevent sweat gland secretions [2]. In some cases, treatment may not be necessary; apocrine chromhidrosis tends to begin after puberty and may regress with age [6].
References
1. Barankin B, Alanen K, Ting PT, et al. Bilateral facial apocrine chromhidrosis. J Drugs Dermatol. 2004; 3(2): 184-6. PubMed2. Matarasso SL. Treatment of facial chromhidrosis with botulinum toxin type A. J Am Acad Dermatol. 2005; 52: 89-91. PubMed
3. Wu JM, Mamelak AJ, Nussbaum R, et al. Botulinum toxin A in the treatment of chromhidrosis. Dermatol Surg. 2005; 31(8Pt 1): 963-5. PubMed
4. Marks JG Jr, Treatment of apocrine chromhidrosis with topical capsaicin. J Am Acad Dermatol. 1989; 21 (2Pt2): 418-20.
5. Malis-Gerrits MM, Van de Kerkhof PC, Mier PD, Happle R. Axillary apocirne chromhidrosis. Arch Dermatol. 1988; 124: 494-6. PubMed
6. Saff DM, Owens R, Kahn TA. Apocrine chromhidrosis involving the areolae in a 15 year-old amateur figure skater. Pediatr Dermatol. 1995; 12: 48-50. PubMed
© 2007 Dermatology Online Journal