Disseminated Lyme Borreliosis preceded by hepatitis in an African American male
Published Web Location
https://doi.org/10.5070/D39d7813rhMain Content
Disseminated Lyme Borreliosis preceded by hepatitis in an African American male
Ramin Fathi1 BA, William Wei-ting Huang2 MD MPH, Katherine Brown1 MD
Dermatology Online Journal 18 (10): 4
1. Rush University Medical Center, Chicago, Illinois2. Wake Forest Baptist Medical Center, Department of Dermatology, Winston-Salem, North Carolina
Abstract
Lyme disease is the most common tick-borne disease in the United States and has a multitude of systemic effects. Infrequently, however, Lyme disease is seen to cause liver dysfunction. Dermatologists should be aware that early, disseminated borreliosis can present with multiple erythema migrans plaques and hepatitis.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. 40-year-old African-American male with erythema migrans on his abdomen. Figure 2. Erythema migrans presentation on the proximal lower extremities. | |
 |
| Figure 3 |
|---|
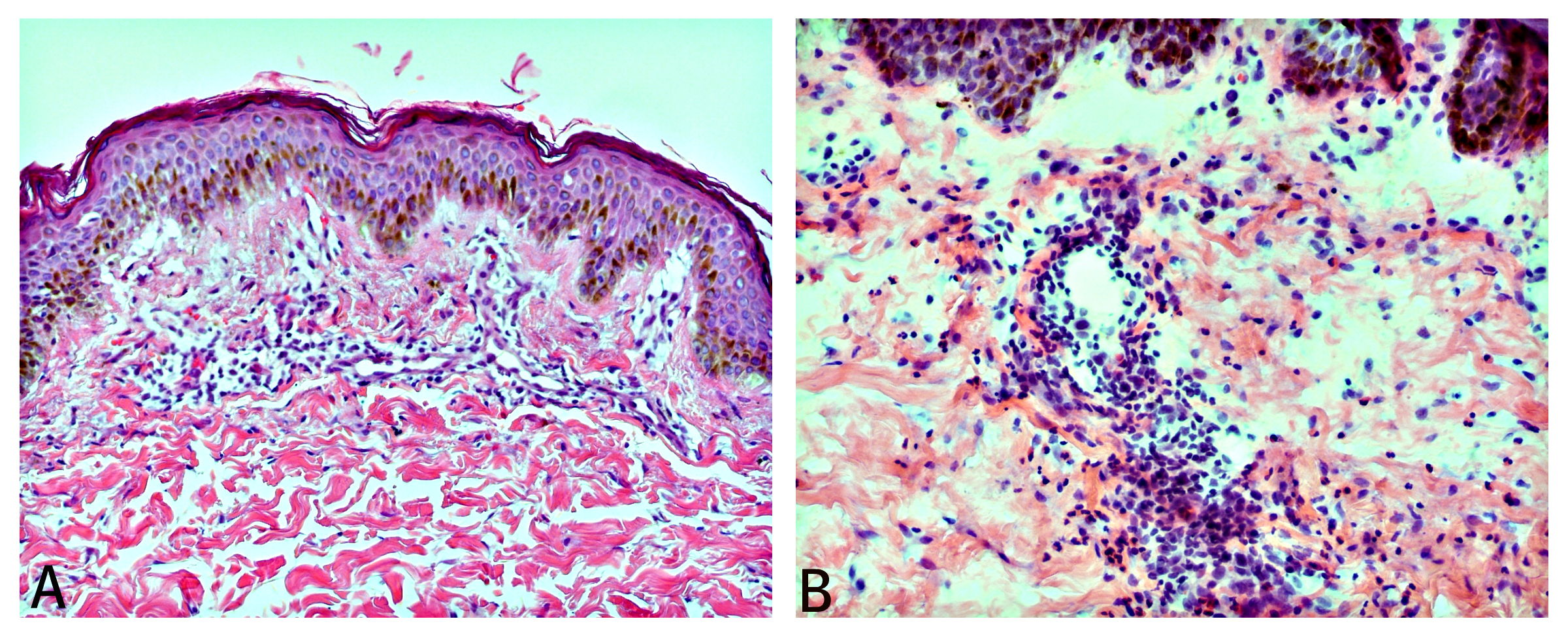
| Figure 3. (A) Punch biopsy of the left thigh showing superficial to mid-dermal moderate perivascular infiltrate consisting of lymphocytes with rare neutrophils (H&E x20). (B) Punch biopsy of the abdomen showing similar spectrum of changes as the left thigh (H&E x40). |
A 40-year-old African-American male presented with a one-week history of diffuse non-scaling annular and polycyclic erythematous plaques with dusky centers ranging from 4 to 12 cm in diameter (Figure 1 and Figure 2). Review of systems was remarkable for headaches, arthralgias, and fatigue. New medications included ibuprofen for headaches one day prior to the onset of the eruption. The patient denied recent travel or outdoor exposures. Three weeks prior to the onset of the eruption he was admitted to the hospital for complaints of fever and malaise and was incidentally found to have a transaminitis: total bilirubin, 5.0 mg/dL (reference range 0.2 – 1.3 mg/dL); alkaline phosphatase, 240 units/L (reference range 30 – 125 units/L); AST, 190 units/L (reference range 3 – 44 units/L); ALT, 360 units/L (reference range 0 – 44 units/L). Abdominal CT and ultrasound, chest x-ray, lab workup, and a hepatology consult were inconclusive in finding a cause and liver enzymes were at near normal levels at the time of eruption onset. Punch biopsies of the left thigh and abdomen were performed (Figure 3).
Histopathologic examination of a 4 mm punch biopsy taken from the left thigh showed superficial to mid-dermal moderate perivascular infiltrate consisting of lymphocytes with rare neutrophils. Lyme titers and an EKG were ordered based on clinical suspicion and the patient was started on doxycycline 100 mg twice daily. Confirmatory ELISA analysis showed elevated Borrelia burgdorferi IgG and IgM antibodies. Confirmatory Western blot analysis revealed antibodies to p18, p23, p39, p41, p45, p58, and p66, which meets the criteria for both positive Lyme IgG IB and Lyme IgM IB by the Center for Disease Control and Prevention [1].
Further interviewing revealed that the patient had recently visited his children in a “wooded area” in Indiana, although he denied having a known exposure to any tick bite. Upon diagnosis of disseminated Lyme disease, the patient was referred to the infectious disease department for further management considerations. At his one-week follow-up, the patient reported resolution of his headaches and arthralgias, and his skin plaques had faded to residual hyperpigmentation.
Comment
Lyme disease, the most common tick-borne disease in the United States, is caused by the spirochete Borrelia burgdorferi. The disease is transmitted to humans through the bite of the vector, various species of the genus Ixodes. Early localized infections present with an expanding annular eruption with a bulls-eye appearance (erythema migrans) accompanied by non-specific complaints of fevers, chills, malaise, fatigue, and headache [2]. Early dissemination presents with multiple erythema migrans lesions, typically within a few days to weeks after contact with the infected tick. Musculoskeletal symptoms including migratory joint or muscle pain (60%), neurologic symptoms including meningitis, radicular neuropathies or facial nerve paralysis (15%), and cardiovascular symptoms including atrioventricular blockades (8%) may be present [3, 4, 5, 6]. If untreated, progression to late dissemination with joint pain and swelling in the knees or hips, chronic neuropathy and encephalopathy, and rarely death may occur [2]. The clinical manifestations of the three stages of North American Lyme disease are summarized in Table 1 [7]. Data suggests that 66 percent of patients with disseminated infections and 34 percent with localized disease have elevated liver function tests, with gamma-glutamyl transferase and alanine aminotransferase as the most common [4]. This association of hepatitis and Lyme disease is more widely reported in the hepatology literature but is not widely discussed in dermatology textbooks or literature.
The diagnosis is based on the presentation of erythema migrans and systemic symptoms. If it is unclear, two-tier testing using the enzyme-linked immunosorbent assay (ELISA) and Western blot to Borrelia burgdorferi IgM or IgG is indicated [2]. A positive Western blot requires IgM to be positive in at least 2 of 3 specific bands and IgG to be positive in at least 5 of 10 specific bands [1, 2]. Two-tier testing yields a 29 percent sensitivity and a 99 percent specificity in the acute phase of erythema migrans and a 64 percent sensitivity and a 99 percent specificity in the convalescent phase. If arthritis, neurologic, or cardiac abnormalities are present because of Borreliosis, two-tier testing is 100 percent sensitive and 99 percent specific [1].
Treatment includes doxycycline 100 mg orally twice daily for patients of ages 9 or older and amoxicillin 50 mg/kg/day orally for patients less than 9 years of age. Two separate studies have found that cefuroxime axetil 500 mg orally twice daily compares favorably in efficacy with doxycycline [8, 9]. Because of the prohibitive cost of cefuroxime axetil, it is regarded as second-line treatment [10]. Early localized infections should be treated for at least 14 days, early disseminated infections for at least 21 days, and Lyme-associated arthritis for 30-60 days. Patients with late or severe disease may require intravenous antibiotics such as ceftriaxone, cefotaxime, or Penicillin G [2, 11].
References
1. Steere AC, McHugh G, Damle N, Sikand VK. Prospective study of serologic tests for Lyme disease. Clin Infect Dis. 2008 Jul 15;47(2):188-95. [PubMed]2. Bratton RL, Whiteside JW, Hovan MJ, Engle RL, Edwards FD. Diagnosis and treatment of Lyme disease. Mayo Clin Proc. 2008 May; 83(5):566-71. [PubMed]
3. Lelovas P, Dontas I, Bassiakou E, Xanthos T. Cardiac implications of Lyme disease, diagnosis and therapeutic approach. Int J Cardiol. 2008 Sep 16; 129(1): 15-21. Epub 2008 May 27 [PubMed]
4. Benedix F, Weide B, Broekaert S, Metzler G, Frick JS, Burgdorf WH, Rocken M, Schaller M. Early disseminated borreliosis with multiple erythema migrans and elevated liver enzymes: case report and literature review. Acta Derm Venereol. 2007; 87(5):418-21. [PubMed]
5. Salzman BE, Stonehouse A, Studdiford J. Late diagnosis of early disseminated Lyme disease: perplexing symptoms in a gardener. J Am Board Fam Med. 2008 May-Jun;21(3):234-6. [PubMed]
6. Shadick NA, Phillips CB, Sangha O, Logigian EL, Kaplan RF, Wright EA, Fossel AH, Fossel K, Berardi V, Lew RA, Liang MH. Musculoskeletal and neurologic outcomes in patients with previously treated Lyme disease. Ann Intern Med. 1999 Dec 21;131(12):919-26. [PubMed]
7. Bhate C, Schwartz RA. Lyme disease: Part I. Advances and perspectives. J Am Acad Dermatol 2011;64:619-36. [PubMed]
8. Nadelman RB, Luger SW, Frank E, Wisniewski M, Collins JJ, Wormser GP. Comparison of cefuroxime axetil and doxycycline in the treatment of early Lyme disease. Ann Intern Med 1992;117:273-80. [PubMed]
9. Luger SW, Paparone P, Wormser GP, Nadelman RB, Grunwaldt E, Gomez G, et al. Comparison of cefuroxime axetil and doxycycline in treatment of patients with early Lyme disease associated with erythema migrans. Antimicrob Agents Chemother 1995;39:661-7. [PubMed]
10. Bhate C, Schwartz RA. Lyme disease: Part II. Management and prevention. J Am Acad Dermatol 2011;64:639-53. [PubMed]
11. Oksi J, Nikoskelainen J, Hiekkanen H, Lauhio A, Peltomaa M, Pitkaranta A, Nyman D, Granlund H, Carlsson SA, Seppala I, Valtonen V, Viljanen M. Duration of antibiotic treatment in disseminated Lyme borreliosis: a double-blind, randomized, placebo-controlled, multicenter clinical study. Eur J Clin Microbiol Infect Dis. 2007 Aug;26(8):571-81. [PubMed]
© 2012 Dermatology Online Journal