Median raphe cyst of the penis
Published Web Location
https://doi.org/10.5070/D39bq5f4ckMain Content
Median raphe cyst of the penis
Raquel Cardoso MD , João Duarte Freitas MD, José Pedro Reis MD, Óscar Tellechea PhD
Dermatology Online Journal 11 (3): 37
Department of Dermatology, University Hospital, Coimbra, Portugal. raquel.tavares.cardoso@ iol.pt
Abstract
Cysts of the median raphe are uncommon. We describe a 43-year-old man with an asymptomatic nodule on the glans penis. Excision of the lesion was performed followed by histological and immunohistochemical studies. Histopathological examination revealed a solitary unilocular cystic cavity in the corium, lined by a pseudostratified columnar epithelium, among which mucinous cells where identified. Hints of decapitation secretion occurred at the apex of the luminal layer. An immunohistochemical study using a standard avidin-biotin peroxidase method disclosed CK7 and CK13 reactivity in the columnar cells. Epithelial membrane antigen (EMA) and carcinoembrionyc (CEA) antigen immunoreactivity occurred at the apical border of the luminal cells. No staining was obtained with anti-CK20, human milk fat globulin 1 (HMFG1) and anti- S100 protein. The study supports its histogenetic relationship with the urothelium.
Introduction
Cysts of the median raphe are midline-developmental cysts that can occur anywhere from the anus to the urinary meatus [1, 2]; when located on the border of the meatus they are also known as parameatal cysts [3]. Most are present from birth and remain undetectable until adolescence or adulthood, occurring as a solitary freely movable nodule on the ventral surface of the penis [2].
In general the lesion is asymptomatic and does not interfere with urinary or sexual function [2]. Trauma and infection can complicate the picture [4].
Histologically the cyst does not communicate with the urethra; it is lined by a pseudostratified, columnar or stratified squamous cell epithelium, similar to urethral transitional epithelium [2, 5]. The luminal cells may present with what appears to be decapitation secretion; as a result, the lesion can be misinterpreted as an apocrine hydrocystoma or cystadenoma [6, 7].
Cysts of the median raphe are thought to arise from embryologic developmental defects of the male urethra [1, 2, 3].
We report a case in which a immunohistochemical study was performed; it was unusual for the sudden growth in the absence of inflammatory signs or trauma.
Clinical synopsis
A 43-year-old man presented with an asymptomatic nodule on the glans penis (Figs. 1, 2). The lesion was first noticed at adolescence as a tiny nodule. It remained unchanged until recently when it suddenly increased in size leading the patient to seek medical attention. There was no history of trauma, local subjective symptoms, or application of topical medications. Observation showed a 1.0 cm x 0.7 cm, smooth, soft, painless nodule, covered by normal skin located on the ventral surface of the penis (Figs. 1 and 2). No inflammatory signs were present.
The lesion was surgically removed (Fig. 3).

|

|
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Median raphe cyst of the penis. | |
| Figure 2. Close view of the lesion. | |

|
|
| Figure 3 | Figure 4 |
|---|---|
| Figure 3. After cyst excision | |
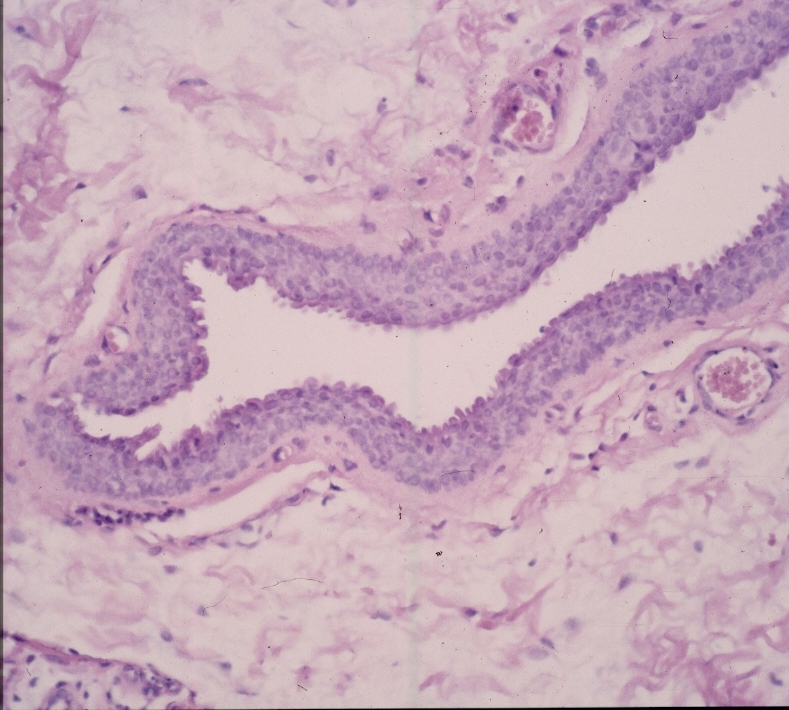
| Figure 4. Cystic cavity layered by pseudostratified columnar epithelium (H-E; 40 ×) | |
Histopathological examination revealed a solitary unilocular cystic cavity in the corium, lined by a pseudostratified columnar epithelium of varying thickness and with occasional large, mucinous cells (Figs. 4 and 5). Hints of decapitation secretion occurred at the apex of the luminal layer (Fig. 5). The lumen appeared empty. Atypia and inflammatory infiltrate were absent (Figs. 4 and 5).

|

|
| Figure 5 | Figure 6 |
|---|---|
| Figure 5. Note single larger mucinous cell within the epithelium and hints of decapitation secretion in the apical border of luminal cells (H-E 40 ×). | |
| Figure 6. Apical cells were diffusely stained by CK 7. | |
An immunohistochemical study using a standard avidin-biotin peroxidase method disclosed CK7 and CK13 reactivity in the columnar cells (Figs. 6 and 7). Epithelial membrane antigen (EMA) and carcinoembrionyc (CEA) antigen immunoreactivity occurred at the apical border of the luminal cells (Fig. 8). No staining was obtained with anti-CK20, human milk fat globulin 1(HMFG1) and anti- S100 protein.
No recurrence was observed at a 3-year followup examination.

|

|
| Figure 7 | Figure 8 |
|---|---|
| Figure 7. Apical cells were also stained by CK 13. | |
| Figure 8. CEA decorated luminal cells. | |
Discussion
Median raphe cysts of the penis are uncommon benign lesions affecting young men [1, 2]. Several terms including mucus cyst of the penis, genitoperineal cyst of the medium raphe, parameatal cyst, hydrocystoma, and apocrine cystadenoma of the penile shaft have been coined to describe the lesion and should be regarded as synonymous [3].
As in the present case the cysts develop mainly on the ventral surface of the penis [1, 2, 5], mostly near the glans, but can occur anywhere from the urinary meatus to the anus. Rarely they can be pigmented [8] or occur as a perianal polyp [9]. Generally they are asymptomatic but can be complicated by infection or trauma [2] and therefore may be treated by surgical excision.
Clinical differential diagnosis include glomus tumor, dermoid cyst, pilonidal cyst, epidermal cyst, urethral diverticulum, and steatocystoma [2]. All of these were readily differentiated by the histological findings typical of median raphe cyst, a single cystic cavity with no urethral communication and lined by a columnar pseudo-stratified epithelium [1]. Distinguishing median raphe cyst from apocrine hidrocystoma, however, may be less straightforward. In fact, several reports of apocrine cystadenoma of the penis may represent cysts of the median raphe [6, 7]. The absence of a basal layer of cuboidal, myoepithelial cells, and the absence of true decapitation secretion (as pictured in the present case) are important for this distinction [10]. Apocrine cystadenomas, by contrast with our case of median raphe cyst, have an apical border of luminal cells in are regularly stained by anti-HMFG [7], a peripheral layer of S100 protein, and the presence of α-smooth-muscle actin-positive cells [11].
The lining epithelium varies according to the to the segment origin of the urethra of the lesion, i.e., stratified in the distal part (ectodermal origin) and columnar pseudostratified in the remainder of the urethra (endodermal origin) [2].
Median raphe cyst is considered an embryologic developmental abnormality of the male genitalia [1, 2, 9]. Different histogenetic explanations have been suggested including incomplete fusion of the urethral folds, abnormal formation of epithelial buds from the urethral epithelium that then became sequestrated and independent after closure of the medium raphe, and cystic dilatations of ectopic Littré's periurethral glands [2, 3].
Although the cytokeratin pattern we observed, with CK 13 and 17 positivity in the lining cells, that concurs with that found in other studies [12], suggests the urethral origin of the cyst, it cannot distinguish among these possibilities.
The absence of CK20 immunoreactivity also reported in medium raphe cyst of the penis by Dini et al. [13], contrasts with the well known expression of this intermediate filament in urethral neoplasms [14, 15] and may be related to the benign, non-dysplastic nature of the lesion [14, 15].
In conclusion, we have presented a medium raphe cyst case with sudden growth in the absence of a precipitating factor or inflammation whose study supports its histogenetic relationship with the urothelium.
origin in the urethral epithelial remains, resulting from an ; ii)
in contrast with the findings in the present case,
References
1. Kirkham N . Tumors and cysts of the epidermis. In Elder D, Elenitsas R, Jasorsky C, Jonhson B (eds.). Lever's Histopatology of Lever; Lippincott-Raven, Philadelphia, 8th edn., 1997 : 685-746.2. Nagore E, Sanchez-Motilla JM, Febrer MI, Aliaga A. Median raphe cysts of the penis: a report of five cases. Pediatric Dermatology 1998; 15(3): 191-193.
3. Otsuka T, Ueda Y, Terauchi M, Kinoshita Y. Median raphe (parameatal) cysts of the penis. J Urol 1998 Jun; 159(6): 1918-20.
4. Soendjojo A, Pndha S. Trichomonas vaginalis infection of the median raphe of the penis. Sex Transm Dis 1981 0ct-Dec; 8(4): 255-7.
5. Romani J, Barnadas MA, Miralles J et al. Median raphe cyst of the penis with ciliated cells. J Cutan Pathol 1995 Aug; 22 (4): 378-81.
6. Terau Y, Hamada T. Median raphe cyst of the penis. Cutis 1984 Nov; 34 (5): 495-496.
7. Onishi T, Watanabe S. Immunohistochemical analysis of Human milk fat globulin 1 and cytokeratin expression in medium raphe cyst of the penis. Clin Exp. Dermatol 2001; 26: 88-92.
8. Urashi J., Hara H., Yamaguchi Z, Morishima T. Pigmented raphe cysts of the penis. Acta Derm Venereol 2000; 80:297-298
9. Scelwyn M. Median raphe cyst of the perineum presenting as a perianal polyp. Pathology 1996; 28: 201-202.
10. Elder D, Elenitsas R, Ragsdale BD. Tumors of the epidermal appendages. In Elder D, Elenitsas R, Jasorsky C, Jonhson B (eds.). Lever's Histopatology of Lever; Lippincott-Raven, Philadelphia, 8th edn., 1997 : 747-803.
11. Eckert F, Betke M, Schmoeckel C, Neuwiler J, Schmid U. Myoepithelial differentiation in benign sweat gland tumors. J. Cutan. Pathol 1992; 19:294-301.
12. Richard-Lallemand MA, Choux R, Szekeres G et al. Characterization immunohistochimique d'un kyste du raphe Ann Pathol 1994; 14: 174-176.
13. Dini M, Baroni G, Colafranceschi M. Medium raphe cyst of the penis: report of two cases with immunohistochemical investigation. Am J Dermatopathol 2001; 23:320-324.
14. Moll R. Cytokeratins and histological diagnosis of malignant tumors. Int J Biol Markers 1994 Apr-Jun; 9(2):63-9.
15. Southgate J, Harnden P, Trejdosiewicz LK. Cytokeratin expression patterns in normal and malignant urothelium: a review of the biological and diagnostic implications. Histol Histopathol 1999 Apr; 14(2): 657-64.
© 2005 Dermatology Online Journal