Acquired dermal melanocytosis of the hand at the site of treated psoriasis
Published Web Location
https://doi.org/10.5070/D39754k03xMain Content
Acquired dermal melanocytosis of the hand at the site of treated psoriasis
Brian P Kelley MD1, Sean D Doherty MD1, Antoanella Calame MD2, Sylvia Hsu MD1
Dermatology Online Journal 15 (12): 2
1. Department of Dermatology, Baylor College of Medicine, Houston, Texas. shsu@bcm.edu2. Department of Dermatology, University of Texas Southwestern Medical Center, Dallas, Texas
Abstract
Dermal melanocytosis is a benign phenomenon most commonly noted in people with darkly pigmented skin. Multiple entities with dermal melanocytosis are described, including Mongolian spot, nevus of Ota, nevus of Ito, nevus of Hori, and acquired dermal melanocytosis. We report a case of acquired dermal melanocytosis occurring in a 42-year-old Hispanic man with psoriasis treated with infliximab for 9 months. The patient presented with an isolated pigmented patch on his left dorsal hand. Histopathologic examination of the skin revealed numerous dendritic, heavily pigmented melanocytes in the papillary and upper reticular dermis. We review the literature and discuss the pathogenesis of acquired dermal melanocytosis.
Introduction
Dermal melanocytosis is an unusual, benign abnormalitiy of skin pigmentation, characterized by the histopathologic presence of dendritic melanocytes in the dermis [1]. Clinically, these lesions are recognizable by their distinctive gray or blue-gray appearance, also known as ceruloderma, which is caused by the Tyndall effect. Most commonly, these lesions are found to be congenital or appear later in childhood or adolescence. Common types of congenital dermal melanocytosis include the Mongolian spot, nevus of Ota, and nevus of Ito, which may be more common in Asian patients [2, 3, 4]. Other lesions include variations of the nevus of Hori and the blue nevus which appear after birth [5, 6]. Nevi of Hori have been further differentiated by location as acquired dermal melanocytosis (ADM), ADM of the face and extremity, nevus fusco-caeruleus zygomaticus, and acquired and symmetrical dermal melanocytosis (ASDM) due to atopic dermatitis [7, 8, 9, 10]. Herein, we report a case of asymmetric ADM restricted to the hand in an adult with psoriasis who had been treated with the tumor necrosis factor-α inhibitor infliximab.
Case report
 |
| Figure 1 |
|---|
| Figure 1. 1.5 cm x 1.2 cm well-circumscribed blue-gray patch on dorsum of left hand. |
A 42-year-old Hispanic man with a 12-year history of severe plaque-type psoriasis covering 80-90 percent of his body presented to clinic with almost complete resolution after five infusions of infliximab. He complained of a dark area on his left hand that he did not remember seeing previously. He thought that the area might have been located in a similar distribution to a previously present psoriatic plaque. On physical examination the patient was noted to have a 1.5 cm x 1.2 cm well-circumscribed blue-gray patch on the dorsum of his left hand (Fig. 1). He had no family history of comparable lesions and the lesion had been asymptomatic.
 |  |
| Figure 2 | Figure 3 |
|---|---|
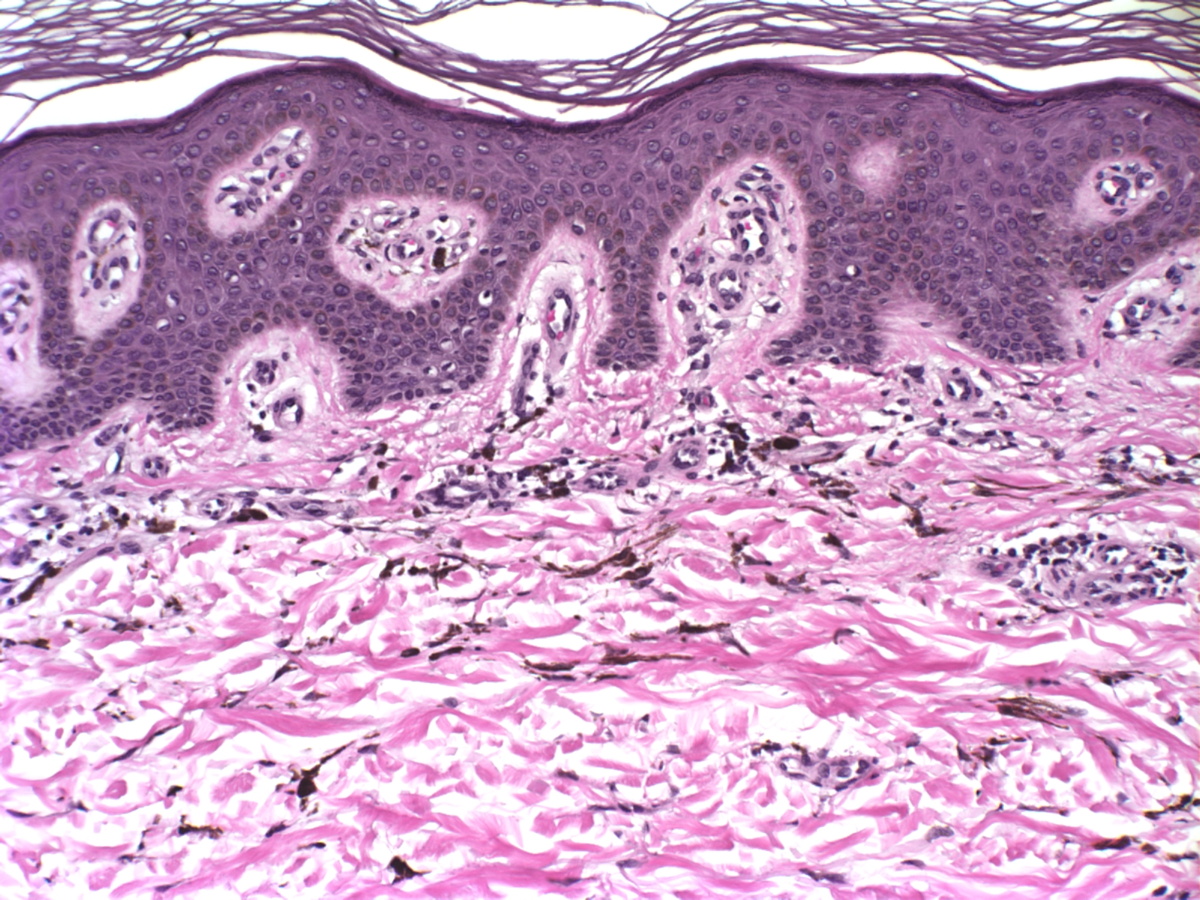
| Figure 2. Numerous, diffusely scattered, dendritic, heavily pigmented melanocytes in the dermis (H&E, x200) Figure 3. Dendritic, heavily pigmented melanocytes in the dermis (H&E, x400) | |
A 4 mm punch biopsy of the lesion was performed and histopathologic examination demonstrated slight epidermal hyperplasia and basal hyperpigmentation with numerous, diffusely scattered, dendritic, heavily pigmented melanocytes (Figs. 2 & 3). There was no increase in the number of melanophages. These histopathologic findings were consistent with dermal melanocytosis.
Discussion
Dermal melanocytosis consists of a diverse group of congenital and acquired lesions. It is often necessary to use clinical correlation in order to appropriately diagnose such lesions because the histopathology shows similar dendritic, dermal melanocytes for all dermal melanocytosis. An exception is the common blue nevus, which has a unique histologic appearance [1].
The clinical diagnosis is commonly defined by a combination of anatomic location, symmetry, appearance, and involvement of cutaneous dermatomes. Mongolian spots are congenital lesions appearing as uniform, blue-gray patches on the sacral and buttocks areas, most commonly in Asian or black infants [2]. Nevus of Ota, also known as oculodermal melanocytosis and nevus fuscocaeruleus ophthalmomaxillaris, is a type of congenital dermal melanocytosis that involves the areas innervated by the first and second divisions of the trigeminal nerve. It appears as speckled or mottled brown-gray to blue-black patches that may involve skin, conjunctiva, sclera, tympanic membrane, or oral and nasal mucosa of the affected dermatomes. In nevus of Ota, hyperpigmentation is present within the first year of life in greater than 50 percent of patients with the remainder presenting by adolescence [3]. Glaucoma develops in approximately 10 percent of patients and ipsilateral sensorineural hearing loss has also been reported [11]. Nevus of Ito, also known as fuscocaeruleus acromiodeltoideus, is another congenital dermal melanocytosis involving skin innervated by the posterior supraclavicular and lateral brachiocutaneous nerves [4]. Otherwise, it is clinically and histopathologically similar to nevus of Ota.
The nevus of Hori was first described in 1984 by Hori et al. and is defined as an acquired, bilateral nevus of Ota-like macules (ABNOM) [5]. Clinically, these nevi have blue-brown to slate-gray mottled hyperpigmentation with a predilection for the malar regions. Similar to the nevus of Ota, there is an Asian and female predominance. A distinct lack of ocular or mucosal involvement differentiates the nevus of Hori from other forms of dermal melanocytosis. Reports have linked sun exposure, hormonal changes in pregnancy, and chronic atopic dermatitis to occurrence of nevi of Hori [5-10].
There are reports of ADM in unusual anatomic locations. To date, few cases of ADM isolated to the extremity have been reported. Most recently, Jimenez et al. described a 60-year-old man with a black-blue patch on his wrist that had appeared at 20 years of age after a bruise to the region [13]. Fukuda el al. described a 22-year-old Japanese man with a 4-year history of ADM of the hand of unknown cause [14]. Pariser et al. reported an ADM in a 24-year-old woman after trauma to the area innervated by the sural nerve [15]. Mevorah et al. described a 32-year-old Portuguese woman who developed a blue macule on the hand that appeared at 11 years of age [8, 10, 16, 17, 18, 19]. Murakami et al. described 12 women and 4 men with ADM on the face and extremities caused by chronic atopic dermatitis [10]. All patients in this report were Japanese.
There are multiple hypotheses for the pathogenesis of acquired dermal melanocytosis [1]. Dermal melanocytosis may represent reactivation of existing dermal melanocytes. This has been supported by the presence of melanocytes in the dermis of uninvolved skin adjacent to lesions [18]. Alternatively, this condition could result from melanocyte descent from the epidermis or migration from the hair bulbs. Finally, it is hypothesized that these lesions could be elicited by dermal inflammation or skin atrophy. Ultimately, the causes of ADM are likely multifactorial and at the present time it is difficult to precisely determine its etiology. The patient presented here may have had a genetic predisposition and may have already had dermal melanocytes present in this area; however, the distribution of the lesion over a patch of recently treated psoriasis makes inflammation in the area a possible factor in the pathogenesis.
References
1. Hori Y, Takayama O. Circumscribed dermal melanoses: classification and histologic features. Dermatol Clinic 1988; 6: 315-326. [PubMed]2. Kikuchi I, Inoue S. Natural history of the Mongolian spot. J Dermatol 1980; 7: 449-450. [PubMed]
3. Ota M, Tanino H. Nevus fusco-caeruleus ophthalmomaxillaris and melanosis bulbi. Tokyo Iji Shinshi 1939; 63: 1243-1245.
4. Ito M. Nevus fusco-caeruleus acromio-deltoideus. Tohoku Exp Med 1954; 60: 10.
5. Hori Y, Kawashima M, Oohara K. Acquired bilateral nevus of Ota-like macules. J Am Acad Dermatol 1984; 10: 961-964. [PubMed]
6. Dorsey CS, Montgomery H. Blue nevus and its distinction from Mongolian spot and the nevus of Ota. J Invest Dermatol 1954; 22: 225-236. [PubMed]
7. Mizoguchi M, Murakami F, Ito M, Asano M, Baba T, Kawa Y, Kubota Y. Clinical, pathological, and etiologic aspects of acquired dermal melanocytosis. Pigment Cell Res 1997; 10: 176. [PubMed]
8. Hidano A, Kaneko K. Acquired dermal melanocytosis of the face and extremities. Br J Dermatol 1991; 124: 96. [PubMed]
9. Sun CC, Lü YC, Lee EF, Nakagawa H. Naevus fusco-caeruleus zygomaticus. Br J Dermatol 1987; 117: 545. [PubMed]
10. Murakami F, Soma Y, Mizoguchi M. Acquired symmetrical dermal melanocytosis (naevus of Hori) developing after aggravated atopic dermatitis. Br J Dermatol 2005; 152: 903. [PubMed]
11. Foster RD, Williams ML, Barkovich AJ, Hoffman WY, Mathes SJ, Frieden IJ. Giant congenital melanocytic nevi: the significance of neurocutaneous melanosis in neurologically asymptomatic children. Plast Reconstr Surg 2001; 107: 933-941. [PubMed]
12. Carney JA, Stratakis CA. Epithelioid blue nevus and psammomatous melanotic schwannoma: the unusual pigmented skin tumors of the Carney complex. Semin Diagn Pathol 1998; 15: 216-224. [PubMed]
13. Jimenez E, Valle P, Villegas C, Roo E, Sanchez Yus E, Furio V. Unusual acquired dermal melanocytosis. J Am Acad Dermatol 1994; 30: 277-278. [PubMed]
14. Fukuda M, Kitajuima J, Fushida H, Hamada T. Acquired dermal melanocytosis of the hand: a new clinical type of dermal melanocytosis. J Dermatol 1993; 20: 561-565. [PubMed]
15. Pariser RJ, Bluemink GG. Acquired linear dermal melanocytosis: nerve course distribution. Arch Dermatol 1982; 118: 125-128. [PubMed]
16. Mevorah B, Frenk E, Delacretaz J. Dermal melanocytosis: report of an unusual case. Dermatologica 1977; 154: 107-114. [PubMed]
17. Buka R, Mauch J, Phelps R, Rudikoff D. Acquired dermal melanocytosis in an African-American: a case report. J Am Acad Dermatol 2000; 43: 934-936. [PubMed]
18. Mizushima J, Nogita T, Higaki Y, Horikoshi T, Kawashima M. Dormant melanocytes in the dermis: do dermal melanocytes of acquired dermal melanocytosis exist from birth? Br J Dermatol 1998; 139: 349-350. [PubMed]
19. Wang W, Fujiwara S, Seguchi S, Yokoyama S, Mizoguchi M. Acquired dermal melanocytosis: a case with conjunctival and gingival pigmentation. J Dermatol 2004; 31: 752-755. [PubMed]
© 2009 Dermatology Online Journal