Another pitfall of sentinel lymph node biopsy: Scar after lymph node biopsy 30 years ago revealed a sentinel lymph node
Published Web Location
https://doi.org/10.5070/D38rk3r29gMain Content
Another pitfall of sentinel lymph node biopsy: Scar after lymph node biopsy 30 years ago revealed a sentinel lymph node
Masami Toya, Miki Tanioka, Hideaki Tanizaki, Akihiro Fujisawa, Yoshiki Miyachi
Dermatology Online Journal 18 (1): 13
Department of Dermatology, Kyoto University Graduate School of Medicine, Kyoto, JapanAbstract
In recent years, sentinel lymph node (SLN) biopsy has been used as a diagnostic and prognostic indicator for a number of tumors, including malignant melanoma. Sentinel lymph node biopsy using combined dye-radiotracer technique improved the detection rate and made the method easier. However, many pitfalls on the SLN procedure have been reported. Herein, we present a new pitfall. A formation of scar and lymph node tissue was detected as a SLN 30 years after lymph node biopsy.
Introduction
In recent years, sentinel lymph node (SLN) biopsy has been used as a diagnostic and prognostic indicator for a number of tumors, including malignant melanoma [1]. Sentinel lymph node biopsy using combined dye-radiotracer technique improved the detection rate and made the method easier. However, many pitfalls on the SLN procedure have been reported. Herein, we present a new pitfall. A formation of scar and lymph node tissue was detected as a SLN 30 years after lymph node biopsy.
 |  |
| Figure 1a | Figure 1b |
|---|---|
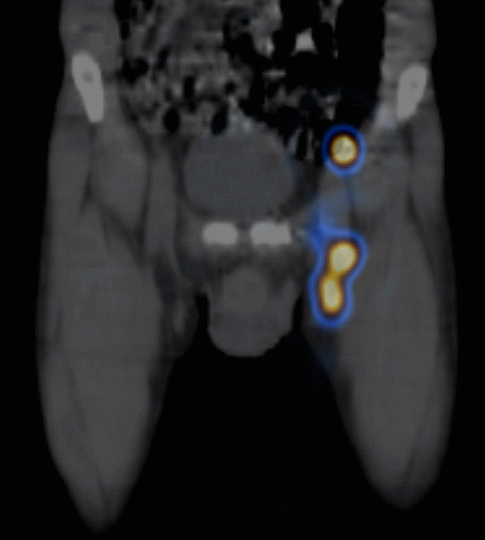
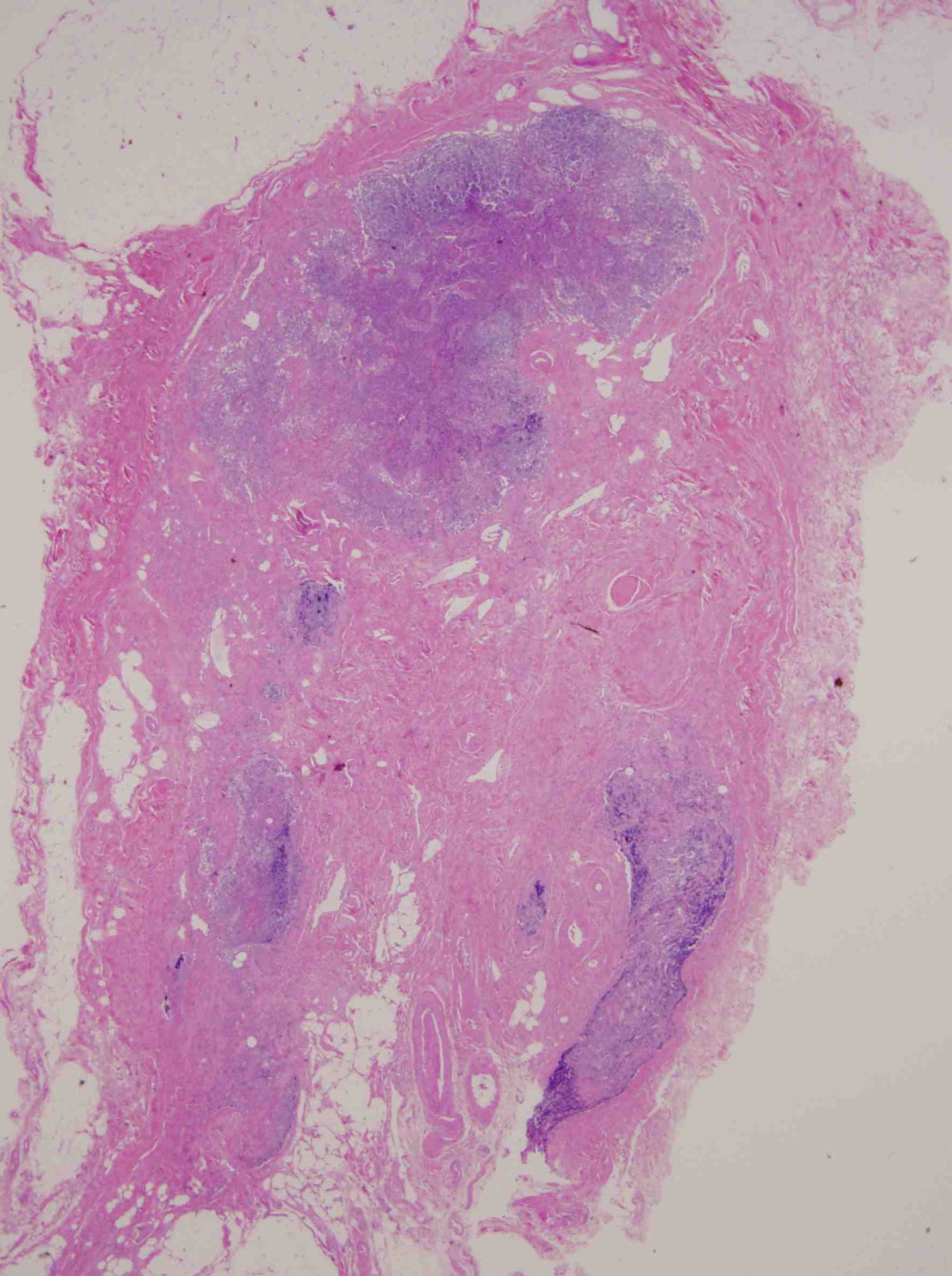
| Figure 1a. SPECT detected two hot spots in the left groin and one hot spot in the lesser pelvis. The distal hot spot matched
the site of a postoperative scar from a lymph node biopsy 30 years prior. Figure 1b. Histopathology of the distal hot spot in SPECT showed a mature scar in the center of the specimen, which was surrounded by lymph node tissue (H&E, x40). | |
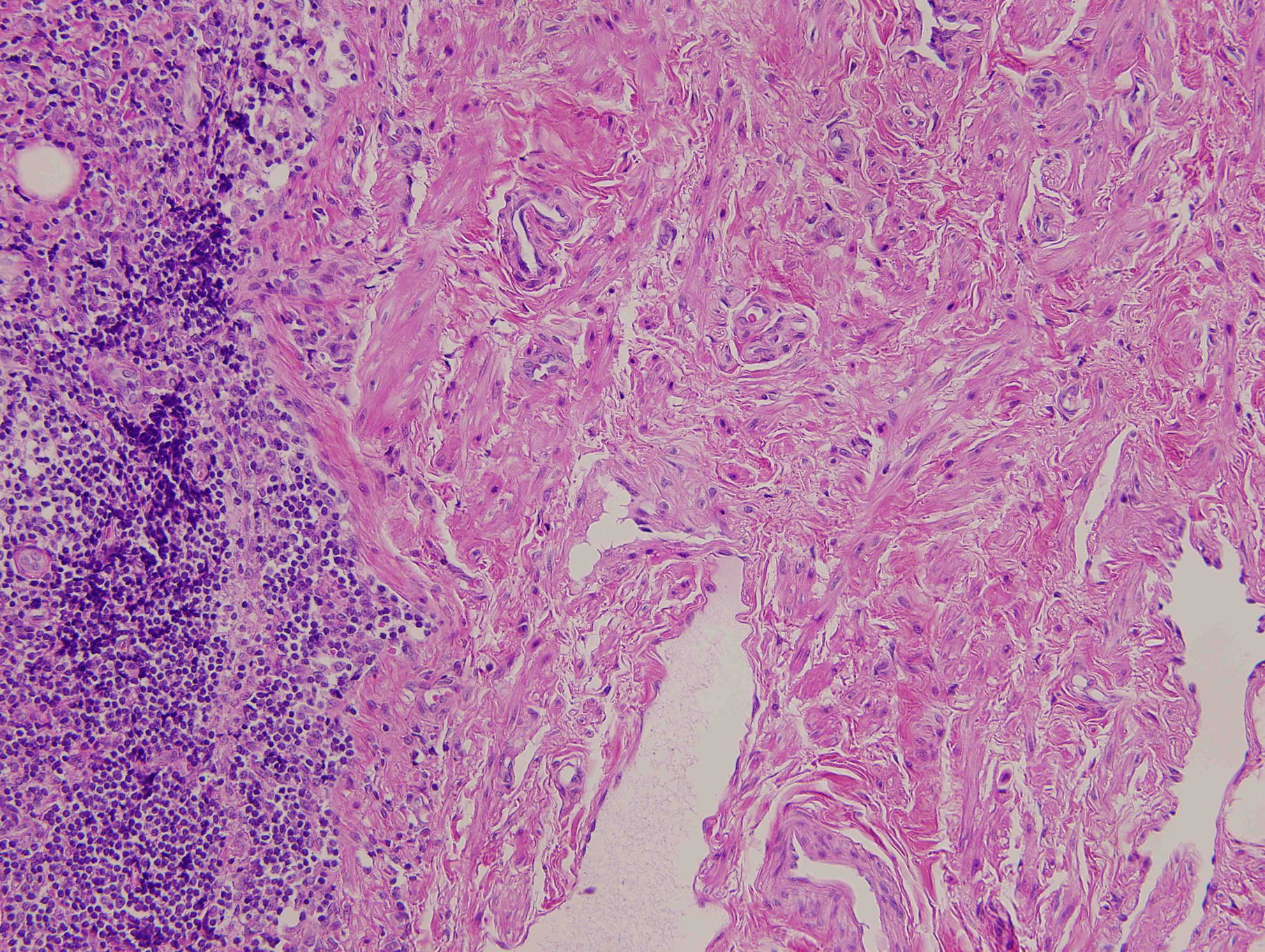 |
| Figure 1c |
|---|
| Figure 1c. High magnification of the boundary of the scar and lymph node tissue (H&E, x200). |
A 61-year-old Japanese male was referred to our hospital for staging and subsequent therapy for malignant melanoma on the left first toe. The primary tumor was removed at a local hospital. The pathology showed the tumor thickness was 1.1 mm. There was no personal or family history of skin malignancies. He had undergone a lymph node biopsy of the left groin 30 years prior because of a suspected lymphoma, which had shown no malignancy and remained as a postoperative scar. For staging of the melanoma, he underwent a SLN biopsy using combined dye-radiotracer technique. Preoperative lymphoscintigraphy combined with CT (SPECT) showed two hot spots in the left groin and one hot spot in the lesser pelvis (Figure 1a). The distal one matched with the postoperative scar of the previous lymph node biopsy. During the SLN biopsy procedure, both a handy gamma probe and blue dye detected the same two sites as positive SLNs. The distal one was a hard subcutaneous mass, which was clinically compatible with scar. Histopathology showed no metastasis in the proximal SLN. In the distal one, lymph node tissue surrounded the postoperative scar, which also showed no metastasis (Figure 1b). We diagnosed the tumor as pT1bN0M0, stage 1B. He went on to receive adjuvant therapy with low-dose interferon beta and no significant adverse effect occurred. He was tumor-free one year after the operation.
Discussion
Sentinel lymph node biopsy is a standard for staging of malignant melanoma. The method is now routinely performed in many institutions. However many pitfalls have been reported. Larn et al reported false-negative SLN biopsy because of obstruction of lymphatics by metastatic melanoma and stressed the value of ultrasound combined with preoperative lymphoscintigraphy [2]. Rokutanda et al also reported a case of false-negative SLN biopsy showing isolated retromammary lymph node metastasis of breast cancer without axillary lymph node involvement [3]. In our case, the postoperative scar was positive in both SPECT and dye tracer. At the time of preoperative scintigraphy, we thought that the hot spot just in the scar might be a false-positive in SPECT. However, during the SLN biopsy, blue dye also was present in the scar. These clinical findings led us to examine the scar as a SLN and histopathology confirmed the lymph node tissue around the scar. We speculated that lymphatic vessel recanalization might occur around the scar. Ikomi et al reported that mature collecting lymphatics are able to regenerate in the adult tissue in rabbits [4]. Tammela et al reported that collecting lymphatic vessels can be regenerated and fused to lymph node transplants after lymph node removal in a mouse model [5]. These studies indicated that recanalization around the postoperative scar from a lymph node biopsy might occur and serve as a route to a SLN.
We should recognize all the possible pitfalls in SLN biopsy and herein, we are reporting a new pitfall. When the combined dye-radiotracer technique shows that a scar is positive, we should examine this area even if the lesion does not look like a normal lymph node clinically.
References
1. Morton DL, Thompson JF, Cochran AJ, et al. Sentinel-node biopsy or nodal observation in melanoma. N Engl J Med 2006; 3551307-17. [PubMed]2. Lam TK, Uren RF, Scolyer RA, et al. False-negative sentinel lymph node biopsy because of obstruction of lymphatics by metastatic melanoma: the value of ultrasound in conjunction with preoperative lymphoscintigraphy. Melanoma Res 2009; 19: 94-9. [PubMed]
3. Rokutanda N, Horiguchi J, Koibuchi Y, et al. Isolated retromammary lymph node metastasis of breast cancer without axillary lymph node involvement: a case report with a false-negative sentinel lymph node biopsy. Breast Cancer 2009; 16: 162-5. [PubMed]
4. Ikomi F, Yokoyama Y, Ogiwara N et al. Recanalization of the collecting lymphatics in rabbit hind leg. Microcirculation 2006; 13: 365-76. [PubMed]
5. Tammela T Saaristo A, Holopainen T, et al. Therapeutic differentiation and maturation of lymphatic vessels after lymph node dissection and transplantation. Nat Med 2007; 13: 1458-66. [PubMed]
© 2012 Dermatology Online Journal