Lupus erythematosus and erythema multiforme-like lesions.
Published Web Location
https://doi.org/10.5070/D38mx006f8Main Content
Lupus erythematosus and erythema multiforme-like lesions.
Rui Mendonca MD
Dermatology Online Journal 3(2): 4
Case ReportA 68 year old female presented in February 1996 with a skin eruption of 10 weeks duration. She initially had sores and bleeding of the lips, and later on developed lesions on the arms, upper chest thighs and legs. Her past medical history included a cerebrovascular accident, hypertension, and an aortic aneurysm. At the time of presentation, her medications included furosemide, digoxin, warfarin, isoptin, potassium, captopril and spironolactone. (The last two had been introduced 3 months prior.)
|
| Physical examination revealed crusted erosions on the lips and annular erythematous plaques on the chest, arms, thighs and legs. The buccal mucosa was not involved.
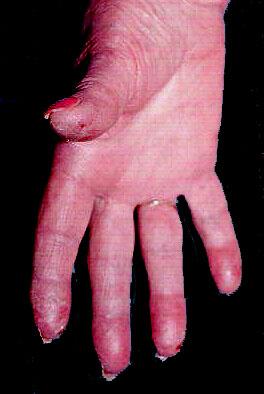
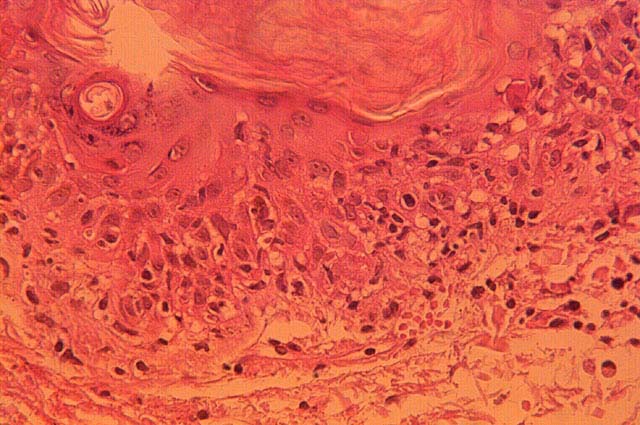
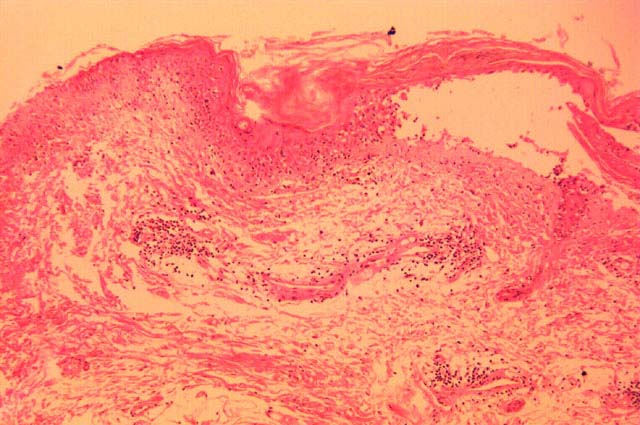
Histopathology of a plaque from the right arm revealed a largely necrotic epidermis with a subepidermal vesicle. Necrotic keratinocytes were present at the dermo-epidermal junction and throughout the epidermis. The upper dermis was edematous and extravasated erythocyes were present and extend into the papillary dermis. The pathology interpretation of the initial biopsy was erythema multiforme. Laboratory examination revealed a positive antinuclear antibody (ANA) 1:640 (speckled), positive anti-DNA antibodies (anti-double stranded DNA) 1:512, and anti-SSB/LA by ELISA of 6.6065 (greater than 3.5 is high positive.) Three months later, the patient continued to develop new skin lesions consisting of targetoid and annular erythematous purpuric plaques on the upper chest, arms, forearms, hands, thighs and legs. Perniotic lesions with ulceration were also present on her fingertips. |
|

|
| Figure 1 | Figure 2 |
|---|
|
Figure 1: Ulcerating purpuric lesions on the fingertips Figure 2: Annular erythematous purpuric plaques on the thighs. |
|
|
| Figure 3 | Figure 4 |
|---|
|
Figures 3 and 4: Histology demonstrating features of erythema multiforme
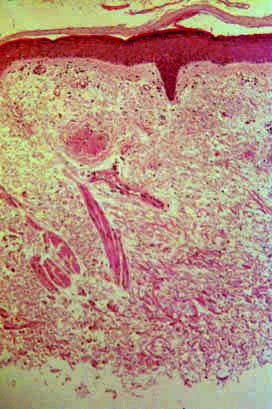
A repeat laboratory evaluation revealed a positive ANA at 1:160, positive anti-DNA antibody at 1:2133, and positive SSB/La antibody at 1:6335. One month later the patient continued to develop new skin lesions, and a second skin biopsy from the right arm revealed basal cell degeneration, edema of the upper dermis, and an increase in vascularity with a patchy mild lymphohistiocytic infiltrate. Some pigmentary incontinence was present. No epidermal necrosis or isolated necrotic cells were identified. The histologic features were interpreted as consistent with a diagnosis of Lupus erythematosus. Subsequent direct and indirect immunofluorescence of lesional and normal skin was not diagnostic. |
|
|
| Figure 5 | Figure 6 |
|---|
|
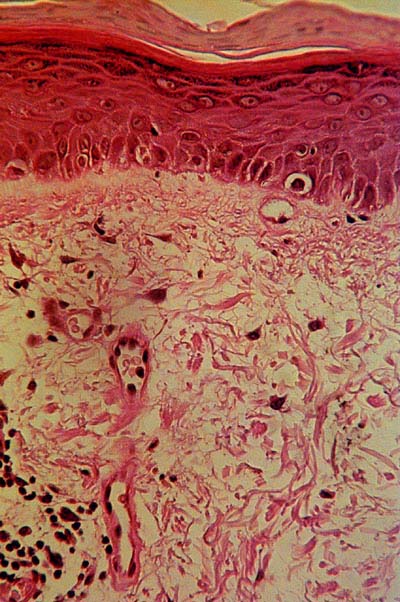
Figures 6 and 7: Histology demonstrating features of lupus erythematosus
The patient initially was treated with topical and oral antibiotics and topical corticosteroids. Two of her most recent chronic medications were changed. Some improvement was noted. However the patient kept relapsing every few weeks. Because of very painful perniosis and the development of new lesions, prednisone was started at the dosage of 10mg twice daily. This was tapered down weekly. She then had clinical remission. answer |