Actinomycetoma by in a girl with Down syndrome
Published Web Location
https://doi.org/10.5070/D381q9w3bbMain Content
Actinomycetoma by Nocardia brasiliensis in a girl with Down syndrome
Martha Pardo1, Alexandro Bonifaz2, Adriana Valencia1, Javier Araiza2, Silvia Anett Mejia1, Carlos Mena-Cedillos1
Dermatology Online Journal 14 (8): 9
1. Dermatology Department, Hospital Infantil de Mexico Federico Gomez. a_bonifaz@yahoo.com.mx2. Mycology Department, Hospital General de Mexico OD
Abstract
We describe the case of a 14-year-old girl with Down syndrome and a large cutaneous plaque localized to the right neck and shoulder that had enlarged over five years after a minor traumatic injury. The plaque was characterized by numerous inflammatory nodules and fistulae that secreted purulent discharge. Nocardia grains were identified and Nocardia brasiliensis was identified by culture. Histopathology examination showed a chronic inflammatory infiltrate with granuloma development. The treatment scheme was with Diaminodiphenylsulfone 50/mg/d and Trimethoprim-Sulfamethoxazole 800/160mg BID. Therapy was continued over 1½ years, with a tapering dose. After 2½ years of continuous treatment, clinical and microbiological healing was achieved.
Introduction
Mycetoma is a chronic condition caused by two types of infectious agents. Eumycetoma is caused by fungi and Actinomycetoma is caused by aerobic filamentous actinomycetes. Mycetoma is a frequent entity in tropical countries. Clinically, it is characterized by its tumorous appearance, draining sinuses, and scarring. The infection most frequently involves the limbs, often extends to the subcutaneous tissue, and easily disseminates to the bones. It is considered an occupational condition [1, 2, 3]. Mycetoma is rarely encountered in children; there are very few reports in the literature. Development of this entity in children is related to exposure to trauma as well as the patient's prevailing health [4, 5, 6]. We report a young patient with Down syndrome who developed actinomycetoma and describe the clinical features and therapeutic response.
Clinical synopsis
 |
| Figure 1 |
|---|
| Figure 1. Clinical case (panoramic) |
A 14-year-old female patient, native and resident of Arcelia Guerrero (400km south of Mexico City), with Down syndrome presented to the Dermatology Department of the Hospital Infantil de Mexico Federico Gomez complaining about progressive skin lesions involving the right side of the neck, thorax, and shoulder. The extensive inflammatory plaque contained erythematous nodules of approximately 0.5 to 1cm in diameter with draining sinuses, crusts, and hypertrophic scars. The onset of the lesions was five years before presentation (at the age of nine) shortly after trauma to the shoulder from a splinter of straw. (Fig. 1)
 |  |
| Figure 2 | Figure 3 |
|---|---|
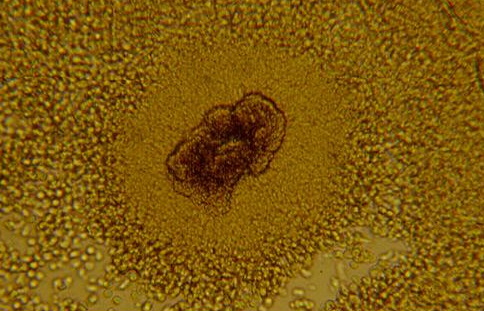
| Figure 2. Nodular lesions with multiple sinuses Figure 3. Granule of Nocardia (Direct examination, Lugol, x20) | |
 |
| Figure 4 |
|---|
| Figure 4. Culture of Nocardia brasiliensis (Sabouraud dextrose agar) |
The initial presumptive diagnosis had been cutaneous tuberculosis and she was treated with anti-tuberculosis therapy (riphampycin + ethambutol) for one year before she was seen at our institution. Some improvement had been noted at the shoulder, but extension had also occurred onto the neck. The presumptive clinical diagnosis in our Dermatology Department was Mycetoma; this was confirmed by means of the following studies: (1) Direct laboratory examination demonstrated multiple lobulated grains or granules that were kidney-shaped, microsyphonated, and approximately 40μm in size with peripheral filaments corresponding to Nocardia sp. Sabouraud dextrose agar cultures demonstrated multiple, dry, rocky colonies and Nocardia brasiliensis was demonstrated by biochemical means. X-rays of the right shoulder showed no bone involvement.
Two skin biopsies were performed. Histopathology findings included epithelial ulceration, crust, and fistulae with acute and chronic inflammatory infiltrate. Granulomas were found in the dermis and subcutaneous areas.
Once the actinomycetoma diagnosis with N. brasiliensis was confirmed, treatment was initiated based upon her weight of 33 kg. Diaminodiphenylsulfone (DDS) 50mg/day and Trimethoprim sulfamethoxazole (TMP/SMZ) 800/160mg BID was initiated. Because of her favorable response after four months the TMP/SMZ dose was decreased by half; DDS was continued at 50mg/day. After 18 months, DDS was discontinued and TMP/SMZ continued for three additional months when clinical and microbiological clearing was confirmed. The patient remained clear when she was examined 2½ years after all medication was stopped.
Discussion
Mycetoma in children is a rare entity and very sporadic cases are reported in the world literature [4-8]. The etiologic agents, both fungi and actinomycetes, have been isolated from the environment where children can come into contact with them through minor trauma. Because the infections are rare, it is assumed, that for the disease to develop, other conditions are required. Most authors consider certain variables to be important, particularly the inoculum size and the patient's immune status [2, 9]. Children in rural areas have more contact with these microorganisms, not only because of their play, but because they often perform agricultural work at a young age. In addition, malnourishment is a common problem among children in rural areas. Eumycetomas, as well as actinomycetoma caused by Nocardia sp., are more common in males. In vitro studies have established that growth of these microorganisms is stimulated by several sex hormones [9]. It is unclear whether these observations are related to the male preponderance of the condition or whether this is mainly related to typical male occupations. However, there is no gender predisposition in children.
The classic presentation of actinomycetoma in children exhibits a tumorous appearance, multiple sinuses, and scarring. Most cases reported a long, slowly progressive disease evolution in children and young adults. A Mexican multicenter study included 2,105 mycetoma reports in a 30-year period. Of the reported cases, 3.7 percent were children under 15 years of age and 0.5 percent were children under 10. Due to the large number of total cases included, this is probably a fairly accurate assessment of the mycetoma frequency in our country [10]. Recently, we have reported 15 cases of mycetomas in children under 15 years of age; a predominance of actinomycetomas was demonstrated [8].
Our patient with Down syndrome manifested the classical presentation of actinomycetoma, similar to that in adults. In addition, our patient did reside in an area endemic for tuberculosis and this led to the incorrect presumptive diagnosis of tuberculosis. However, the slight improvement that she experienced on anti-tuberculosis therapy was probably due to the partial susceptibility of Nocardia brasiliensis to drugs such as rifampicin [6, 8].
Our patient's susceptibility to actinomycetoma was possibly due to the immune suppression associated with Down syndrome. It is known that these patients have various immune defects related to both B and T lymphocyte activities, abnormalities in IgG, IgM and IgA levels, increased infections, increased malignancies, and autoimmune diseases [11, 12, 13, 14].
A well-established treatment for actinomycosis due to Nocardia is DDS and TMP/SMZ and clearing in 1½ years is expected. Our patient's reponse to this treatment is similar to those described earlier [4-8]. Recently, Nolt [15] and Barton [16] reported an excellent therapeutic response in pediatric patients with nocardiosis due to N. brasiliensis with amoxicillin/clavulanate (A/C). The usual dose of A/C for children is 25mg/Kg/day given in divided doses every 12 hours. We have also reported excellent results with A/C in adult patients [17].
References
1. McGinnis MR. Mycetoma. Dematol Clin. 1996; 14(1):97-104. PubMed2. Fahal AH. Mycetoma: a thorn in the flesh. Trans R Soc Trop Med Hyg. 2004; 98(1): 3-11. PubMed
3. Lichon V, Khachemoune A. Mycetoma: a review. Am J Clin Dermatol. 2006; 7(5):315-21. PubMed
4. Aceves Ortega R. Deep mycosis in children. Mod Probl Paediatr. 1975; 17: 228-241. PubMed
5. Welsh O. Mycetoma in children. Mod Probl Paediatr. 1975; 17:248-253. PubMed
6. Pulikot AM, Bapat SS, Tolat S. Mycetoma of the sole. Ann Trop Paediatr. 2002; 22(2): 187-190. PubMed
7. Capoor MR, Khanna G, Nair D, Hasan A, Rajni, Deb M, Aggarwal P. Eumycetoma pedis due to Exophiala jeanselmei. Indian J Med Microbiol 2007; 25(2):155-7. PubMed
8. Bonifaz A, Ibarra G, Saúl A, Paredes-Solis V, Carrasco-Gerard E, Fierro-Arias L. Mycetoma in children. Experience with 15 cases. Pediatr Infect Dis J. 2007; 26(4): 50-52. PubMed
9. Hernández-Hernández F, López-Martínez R, Méndez-Tovar LJ, Manzano-Gayoso P. Nocardia brasiliensis in vitro and in vivo growth response to steroid sex hormones. Mycopathologia. 1995; 132: 79-85. PubMed
10. López R, Méndez LJ, Lavalle P, Welsh O, Saúl A, Macotela-Ruiz E. Epidemiología del micetoma en México: estudio de 2105 casos. Gac Med Mex. 1992; 128(4): 477-481. PubMed
11. Spina CA, Smith D, Korn E, Fahey JL, Grossman HJ. Altered cellular immune functions in patients with Down syndrome. Am J Dis Chile. 1981; 35(3): 251-255. PubMed
12. Lockitch G, Puterman M, Godolphin W, Sheps S, Tingle AJ, Quigley G. Infection and immunity in Down syndrome: a trial of long-term low oral doses of zinc. J Pediatr. 1989; 114(5):781-787. PubMed
13. Lockitch G, Singh VK, Putterman ML, Sheps S, Tingle AJ, Quigley G. Age-related changes in humoral and cell-mediated immunity in Down Syndrome Children living at home. Pediatr Res. 1987; 22(5): 536-540. PubMed
14. Da Rosa Utiyama SR, Nisihara RM, Nass FR, Oliveira NP, Fiedler PT, de Messias-Reason IT. Autoantibodies in patients with Down syndrome: early senescence of the immune system or precocious markers for immunological diseases? J Paediatr Child Health. 2008; 44(4):182-6. PubMed
15. Nolt D, Wadowsky RM, Green M. Lymphocutaneous Nocardia brasiliensis infection: a pediatric case cured with amoxicilin/clavulanate. Pediatr Infect Dis J. 2000; 19(10): 1023-5. PubMed
16. Barton LL. Lymphocutaneous Nocardia brasiliensis infection in children. Pediatr Infect Dis J. 2001; 20(2): 232-233. PubMed
17. Bonifaz A, Flores P, Saul A, Carrasco-Gerard E, Ponce RM. Treatment of actinomycetoma due to Nocardia spp. with amoxicillin-clavulanate. Br J Dermatol. 2007; 156(2):308-11. PubMed
© 2008 Dermatology Online Journal