Lipoid proteinosis: Report of three familial cases
Published Web Location
https://doi.org/10.5070/D37zz4k01rMain Content
Lipoid proteinosis: Report of three familial cases
Amir H Ehsani MD, Maryam Ghiasi MD, and Reza Mahmoud Robati MD
Dermatology Online Journal: 12 (1): 16
Tehran University of Medical sciences, Razi Hospital, Tehran, Iran. robati@razi.tums.ac.irAbstract
Lipoid proteinosis is a rare autosomal recessive disorder; it presents in early childhood with hoarseness, skin infiltration and thickening with beaded papules on eyelid margins, and facial acneiform or pock-like scars. Although 250 cases have been reported until now, the occurrence of disease in siblings is very rare. We report three familial cases of lipoid proteinosis involving a brother and sister and their nephew.
Introduction
Lipoid proteinosis is a rare autosomal-recessive disorder that presents in early childhood with hoarseness, skin infiltration, and thickening, with beaded papules on eyelid margins, and facial acneiform or pock-like scars [1]. Moreover, the respiratory system, upper gastrointestinal tract, CNS, lymph nodes, and stratified muscles sometimes are involved [2]. Histological examinations show an extracellular PAS-positive hyaline material [1, 3]. This disease was first described by Wiethe and Urbach in 1929 and since then about 250 cases are reported. The disorder is attributed to extracellular-matrix protein-1 gene mutation located on chromosome 1q21 [3, 5, 6, 7].
Clinical synopsis
A 19-year-old girl and her 18-year-old brother presented with complaints of papular lesions on the eyelid margins. They stated that these papules have existed since their infancy. Their mother recognized some hoarseness in both of them when they were age 1 year. Moreover, multiple scars developed on their faces. They stated that these scars developed following minor trauma in the preschool ages. There was no history of respiratory difficulties, epilepsy, or other problems. Their parents are not consanguineous. In addition, an 11-year-old nephew has similar hoarseness and eye-lid papules; The hoarseness developed during the first year of life and the eyelid papules developed around age 5.
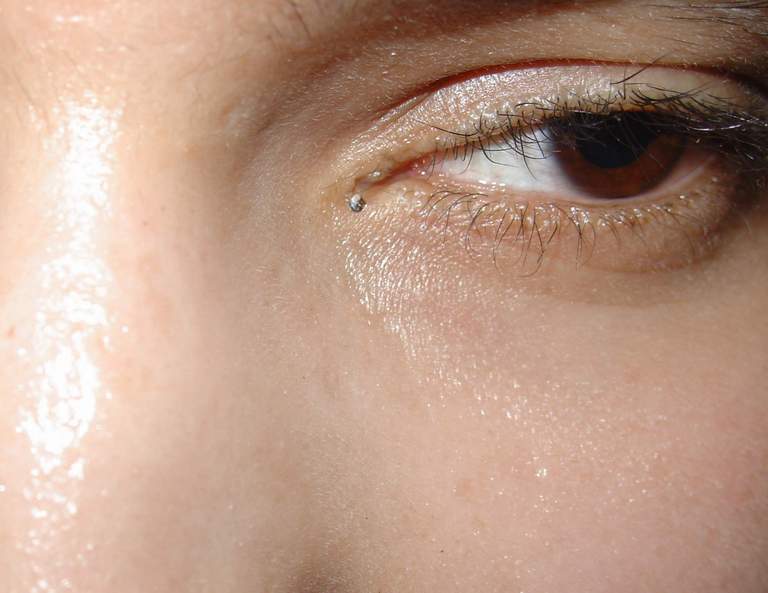
On physical examination, All three patients had hoarseness, but it was most severe in the 11-year-old boy. Bilateral beaded papules were present on the margins of upper and lower eyelids (Figs. 1, 2, 3). Facial acneiform scars, especially on the foreheads and cheeks, were present in all three children; in addition, the 11-year-old boy had scars on the extensor aspects of the arms (Figs. 4, 5, 6). Patients with lipoid proteinosis may develop thickening of the frenulum of tongue, resulting in restriction in protruding of tongue. This finding was most severe in the 18-year-old boy (Fig. 7). Other cutaneous surfaces and mucosal membranes were normal on clinical examinations. Systemic examinations including CNS surveys were normal. Routine laboratory data were reported to be normal in all three patients.
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Beaded papules on the eyelid of the 18-year-old boy. | |
| Figure 2. Beaded papules on the eyelid of the 19-year-old girl. | |
 |  |
| Figure 3 | Figure 4 |
|---|---|
| Figure 3. Beaded papules on the eyelid of the 11-year-old boy. | |
| Figure 4. Pock-like scar on the forehead of the 18-year-old boy. | |
 |  |
| Figure 5 | Figure 6 |
|---|---|
| Figure 5. Pock-like scar on the forehead of the 11-year-old boy. | |
| Figure 6. Pock-like scar on the arm of the 11-year-old boy. | |
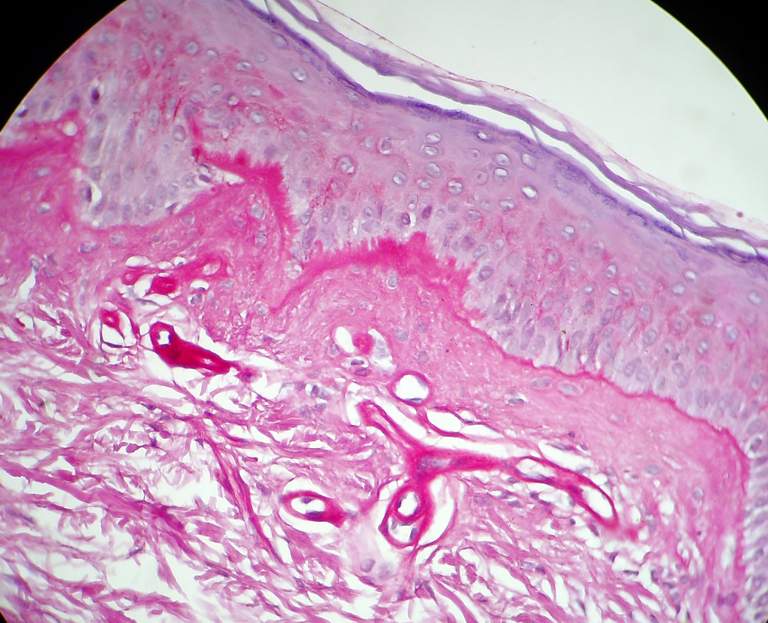
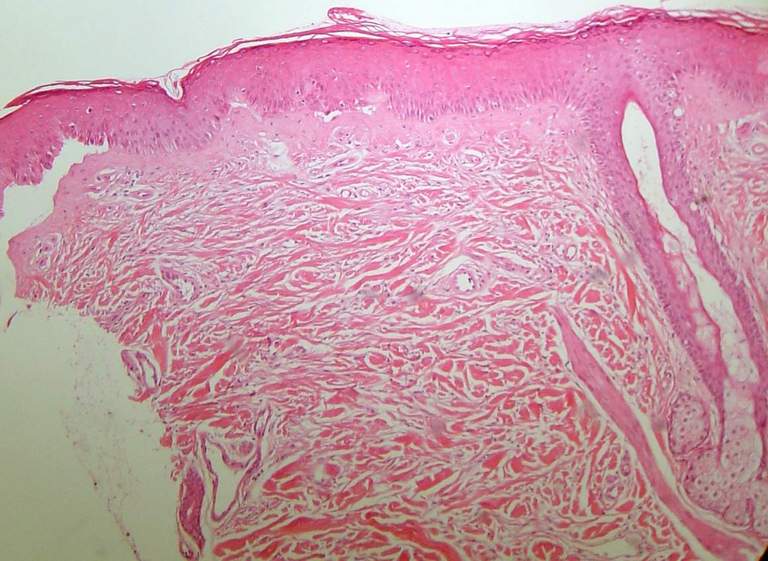
We took a biopsy from one of the eyelid papules in each patient, which showed precipitation of PAS-positive eosinophilic material in the papillary dermis and to some extent in deeper dermis in a similar pattern (Figs. 8, 9).
 |  |
| Figure 7 | Figure 8 |
|---|---|
| Figure 7. Restriction of tongue protrusion in the 18-year-old boy. | |
| Figure 8. Deposition of eosinophilic hyaline material in the papillary dermis (H&E x 100). | |
 |
| Figure 9 |
|---|
| Figure 9. Deposition of eosinophilic hyaline material in the papillary dermis and deeper part of dermis (H&E x 40). |
Discussion
Lipoid proteinosis is a rare autosomal-recessive disorder that presents in early childhood with hoarseness; affected patients subsequently develop skin infiltration and thickening with beaded papules on eyelid margins and facial acneiform or pock-like scars gradually took place [1]. Histological examinations show deposition of extracellular PAS-positive hyaline material [1, 3].
The first symptom of the disease is hoarseness, which is attributed to vocal cord infiltration. It occurs in the majority of patients soon after birth [1]. Laryngeal involvement is usually severe, with nodular lesions on the vocal cords or epiglottis [8]. Skin manifestations present in the first year of life or later. Eyelid beaded papules are the classic cutaneous sign which is easy to diagnose, but sometimes they are very mild and few in number. Other cutaneous manifestations include waxy papules or nodules with yellow hue and generalized skin thickening. Hyperkeratosis may occur in the sites of trauma such as hand, elbow, knee, buttock, and axillae. The skin is vulnerable to trauma in childhood and may form scars. Pock-like or acneiform scars, especially on the face and limbs, are common. Mucous membranes of the pharynx, tongue, soft plate, tonsils, or lip sometimes become infiltrated and this may lead to respiratory difficulty, especially with concurrent respiratory infection. Tracheostomy is sometimes necessary. Scalp involvement is not common, but may result in alopecia. Other probable manifestations include recurrent parotid or submandibular gland swelling, and shortness of tongue attributed to thickening of frenulum [1]. Widespread involvement of internal organs, especially the central nervous system, has been described in this disease and as a fact all organ in body may be affected [9]. In a survey of 29 patients with lipoid proteinosis in South Africa, the most common manifestations were hoarseness and thickening of tongue frenulum [5].
In histological examination the deposition of diastase-resistant, PAS-positive, hyaline-like materials were seen in the dermis [1].
Although 250 cases have been reported to date, occurrence of the disease in siblings is very rare [4, 10]. The most prevalent familial cases were reported in a family with four siblings (two brothers and two daughters) from a nonconsanguineous marriage. All cases show hoarseness and three of them present the typical skin lesions with classic appearance on optical and electronic microscopic evaluation [11]. One report of lipoid proteinosis in a brother and sister found eyelid papules only with no other sign except the histological evaluation was classic for this disease [12].
Although different therapeutic modalities such as systemic steroids, dimethyl sulphoxide, and intralesional heparin injections have been proposed, they are rarely effective. CO2 laser treatment of vocal cords and eyelid papules is helpful for some patients [1]. Etretinate [3] and penicillamine [13] are useful in some cases.
References
1. Hamada T. Lipoid proteinosis. Clin Exp Dermatol. 2002 Nov;27(8):624-9. PubMed.2. Acar A, Eryilmaz A, Gocer C, et al. Lipoid proteinosis of larynx: review of four cases. Int J Pediatr Otorhinolaryngol. 2004 Dec;68(12):1557-61.PubMed.
3. Sarkany RPE, Breathnach SM, Seymour CA, et al. Metabolic and nutritional disorders. In: Burns T, Breathnach S, Cox N, Griffiths C (eds). Rook's textbook of dermatology. Blackwell; 2004:57.1-124.
4. Schivaswamy KN, Thappa DM, Laximish C , et al. Lipoid proteinosis in two siblings: a report from south India. Dermatol online J 2003; 9:12.
5. Van Hougenhouck-Tulleken W , Chan J, Hamada T, et al. Clinical and molecular characterization of lipoid proteinosis in Namaqualand, South Africa. Br J Dermatol. 2004 Aug;151(2):413-23. PubMed.
6. Dereure O. [Mutations in the gene coding for the extra-cellular 1 matricial protein in lipoid proteinosis]. Ann Dermatol Venereol. 2004 Apr;131(4):417 .PubMed.
7. Hamada T, Wessagowit V, South AP, et al. Extra cellular matrix protein 1 gene (ECM1) mutations in Lipoid proteinosis and genotype- phenotype correlation. J Invest Dermatol 2003; 120:345-50.
8. Oz F, Kalekoglu n, Karakullukcu B, et al. Lipoid proteinosis of the larynx. J Laryngol Otol. 2002 Sep;116(9):736-9. PubMed.
9. Al-Bital Y, Samdan AJ. Lipoid proteinosis in two brothers with multiple organ involvement from Saudi Arabia. Int J Dermatol. 2004 May;43(5):360-1. PubMed.
10. Sethuraman G. Tojasvi T, Khaitan BK, et al. Lipoid proteinosis in two siblings: a report from India.J Dermatol. 2003 Jul;30(7):562-5. PubMed.
11. Nanda A, Alsaleh QA, Al-sabah H, et alLipoid proteinosis: a follow-up comment. Pediatr Dermatol. 2002 Mar-Apr;19(2):183-4. PubMed.
12. Sharma V, Kashyap S, Bethria SM, et al. Lipoid proteinosis: a rare disorder with pathognomonic lid lesions. Clin Experiment Ophthalmol. 2004 Feb;32(1):110-2. PubMed.
13. Kaya TI. Kokturk A, Tursen U, et alD-penicillamine treatment for lipoid proteinosis. Pediatr Dermatol. 2002 Jul-Aug;19(4):359-62. PubMed.
© 2006 Dermatology Online Journal