Lichen amyloidosis of the auricular concha: Report of two cases and review of the literature
Published Web Location
https://doi.org/10.5070/D378r2v37cMain Content
Lichen amyloidosis of the auricular concha: Report of two cases and review of the literature
Errol Craig MD PhD
Dermatology Online Journal 12 (5): 1
University of California, Davis Department of Dermatology Abstract
Two cases of lichen amyloidosis of the auricular concha are presented here, supplementing the already approximately twenty cases of lichen amyloidosis of the auricular concha reported to date. The first patient is a 60-year-old woman who presented with a 4-year history of an itchy rash that started in the bowl of her left ear, and soon after appeared on the right side as well. The second patient is a 44-year-old woman who presented with a long-standing pruritic rash on her upper back. This had become noticeably darker over the past several years. In one of the two cases lichen amyloidosis of the auricular concha reported here, concomitant macular amyloidosis of the back was present. Combined cases of lichen and macular amyloidosis are termed biphasic amyloidosis, and provide support to the theory that these two variants of amyloidosis exist on the same disease spectrum.
Clinical synopses
The first patient is a 60-year-old woman who presented with a 4-year history of pruritic lesions that started in the conchal bowl of her left ear, and soon after appeared on the right side as well. She had been treated unsuccessfully with clobetasol ointment, although it somewhat controlled the pruritus. Her past medical history was significant only for hypertension. A family history but not personal history of eczema was noted. Review of systems was unremarkable and negative for alopecia, arthralgia, oral sores, and photosensitivity. Physical exam was remarkable for bilateral, symmetrical brown scaly 1-2 mm monomorphous papules mainly on the conchal bowls (Fig. 1). The clinical impression was discoid lupus erythematosus, and a biopsy sample was taken.
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1: Brown scaly 1-2 mm monomorphous papules in the conchal bowl of patient #1 Figure 2: Rippled hyperpigmented rectangular plaque on the upper back of patient #2 | |
The second patient is a 44-year-old woman who presented with a long-standing pruritic eruption on her upper back, which had become noticeably darker over the past several years (Fig. 2). Physical examination revealed a rippled hyperpigmented rectangular plaque on the upper back, as well as monomorphous shiny brown 1-2 mm papules in the conchal bowl and on the scapha of the right ear (Fig. 3). Biopsies were taken from both the back and the ear for histopathologic analysis.
 |  |
| Figure 3 | Figure 4 |
|---|---|
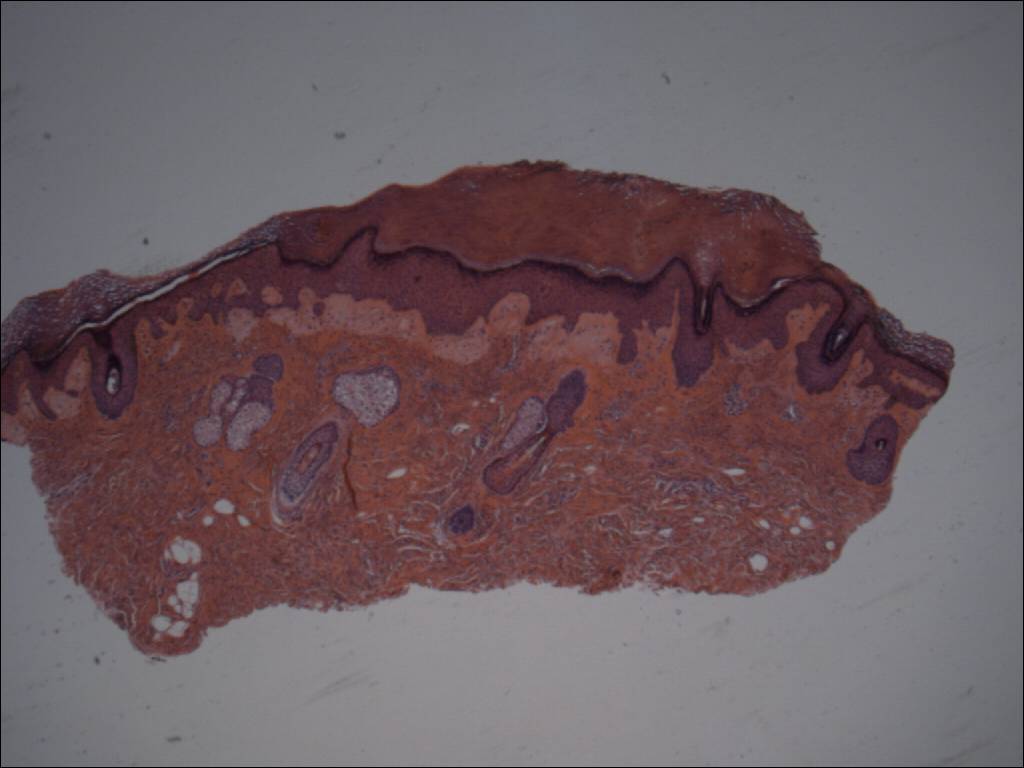
| Figure 3: Monomorphous shiny brown 1-2mm papules in the conchal bowl and on the scapha of the right ear of patient #2 Figure 4: Scanning magnification of an auricular papule as shown in Fig. 1. Acanthosis and hyperkeratosis are evident, as well as a broad band of light staining amorphous material in the papillary dermis. Inflammation is sparse. Hematoxylin and eosin stain; Mag: 40X. | |
 |  |
| Figure 5 | Figure 6 |
|---|---|
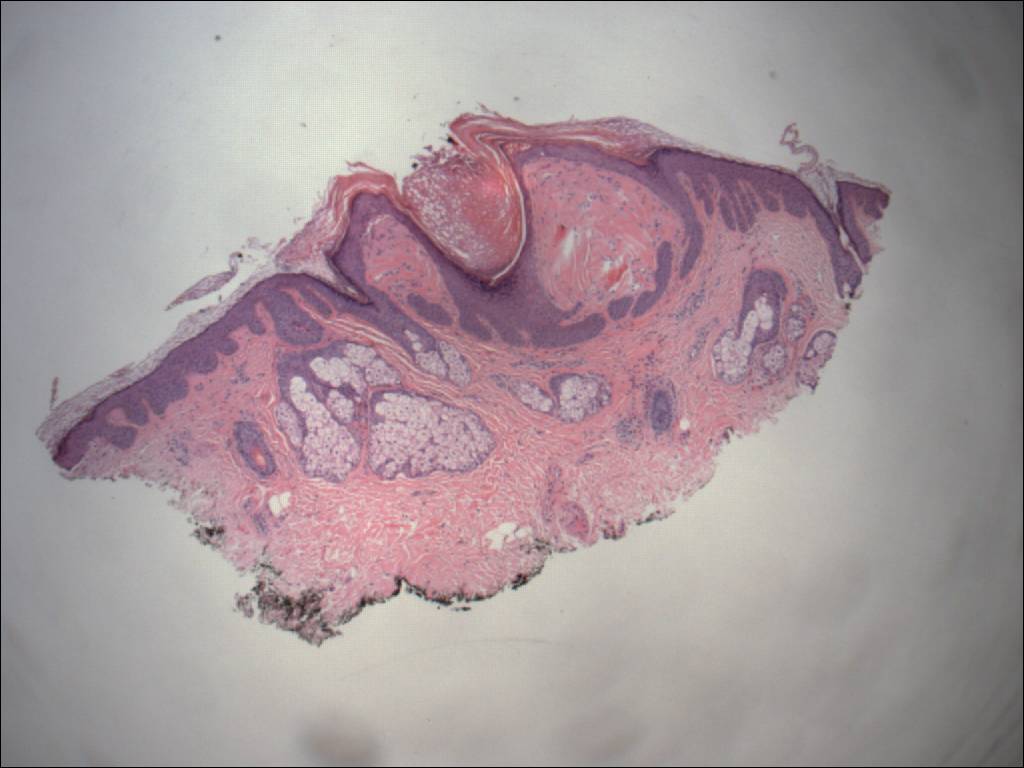
| Figure 5: Scanning magnification of an auricular papule shown in Fig. 3. Follicular plugging is prominent. Acanthosis and
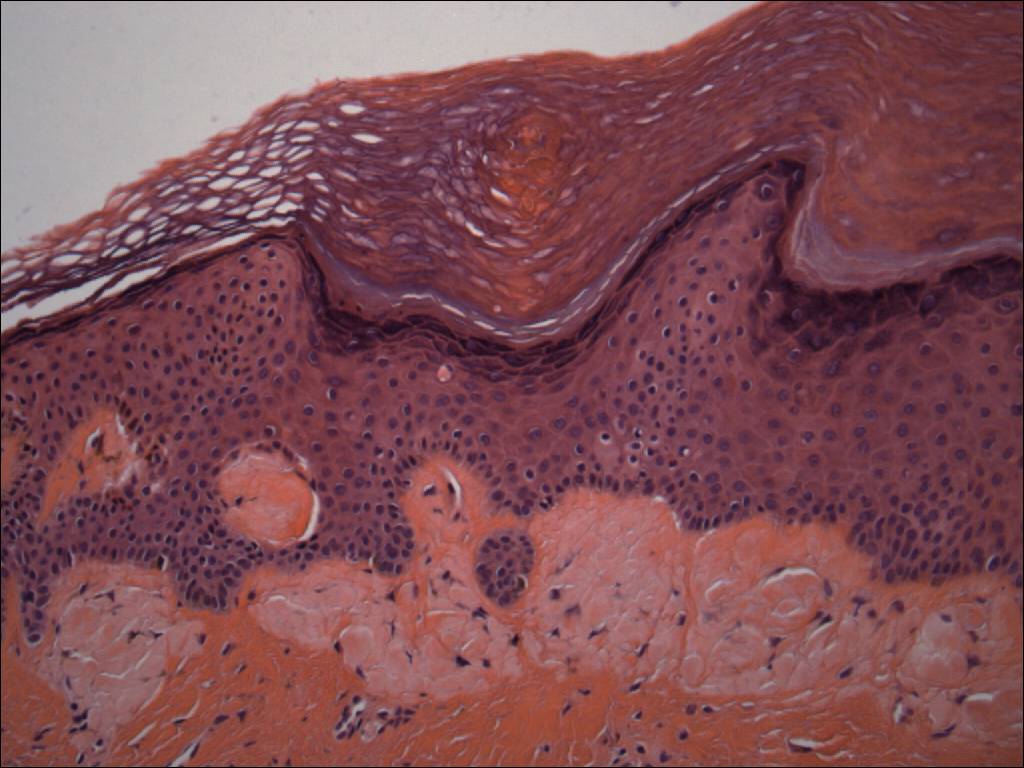
a pauci-inflammatory infiltrate are also present. Hematoxylin and eosin stain; Mag: 40X. Figure 6: Higher magnification of Fig. 4. The pale amorphous material in the papillary dermis appears globular, suggestive of amyloid. Hematoxylin and eosin stain; Mag: 200X. | |
 |  |
| Figure 7 | Figure 8 |
|---|---|
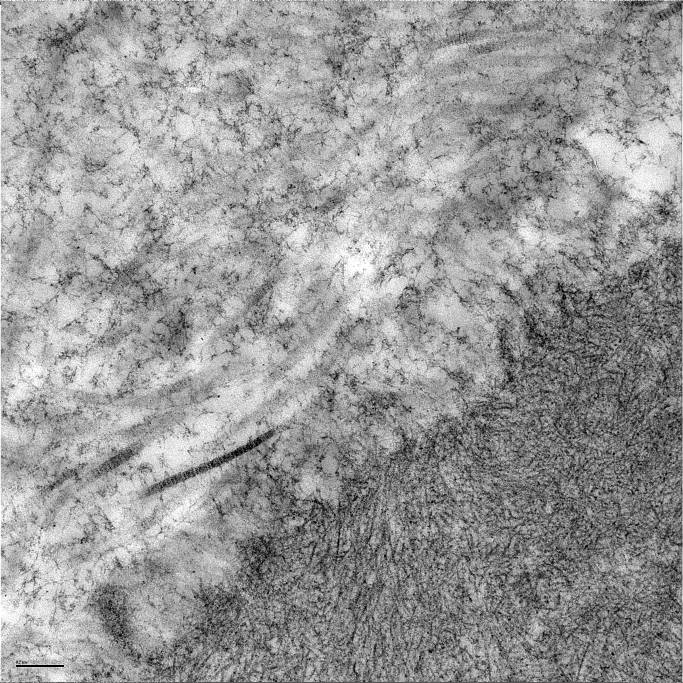
| Figure 7: An electron micrograph of an auricular papule from patient #1. A collection of haphazardly interspersed fibrils
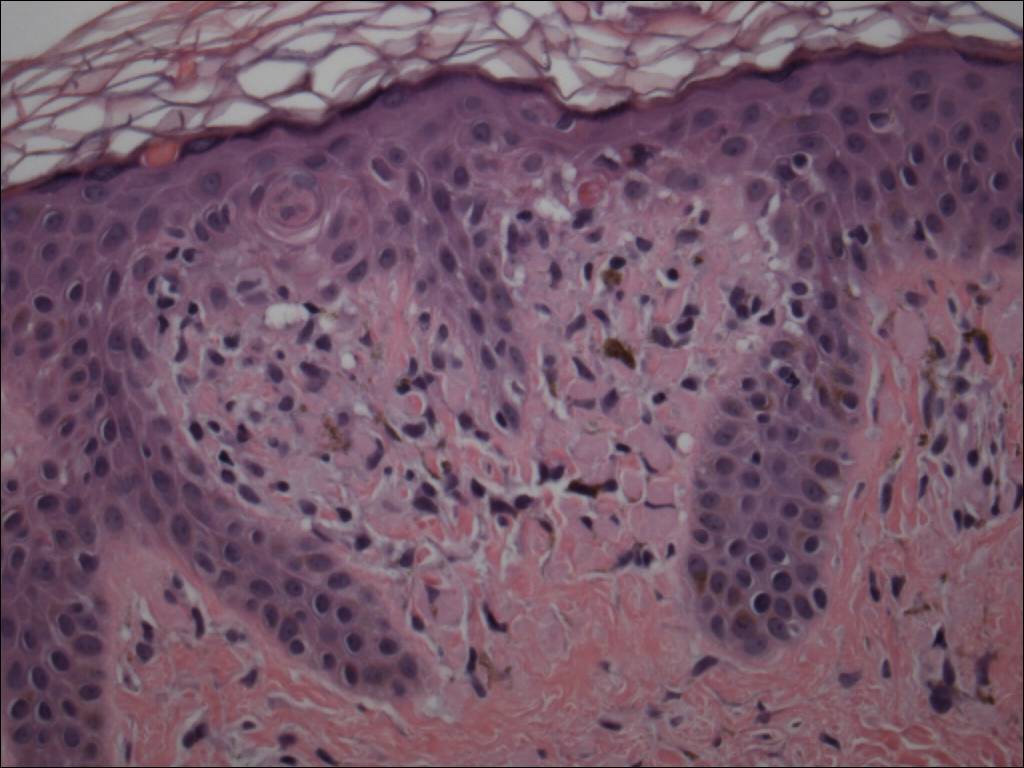
are seen, consistent with amyloid Figure 8: Histopathology of the rippled plaque depicted in Fig. 2. Subtle pink globules are seen filling a dermal papillae with an increased number of mononuclear cells. Hematoxylin and eosin stain; Mag: 400X. | |
 |
| Figure 9 |
|---|
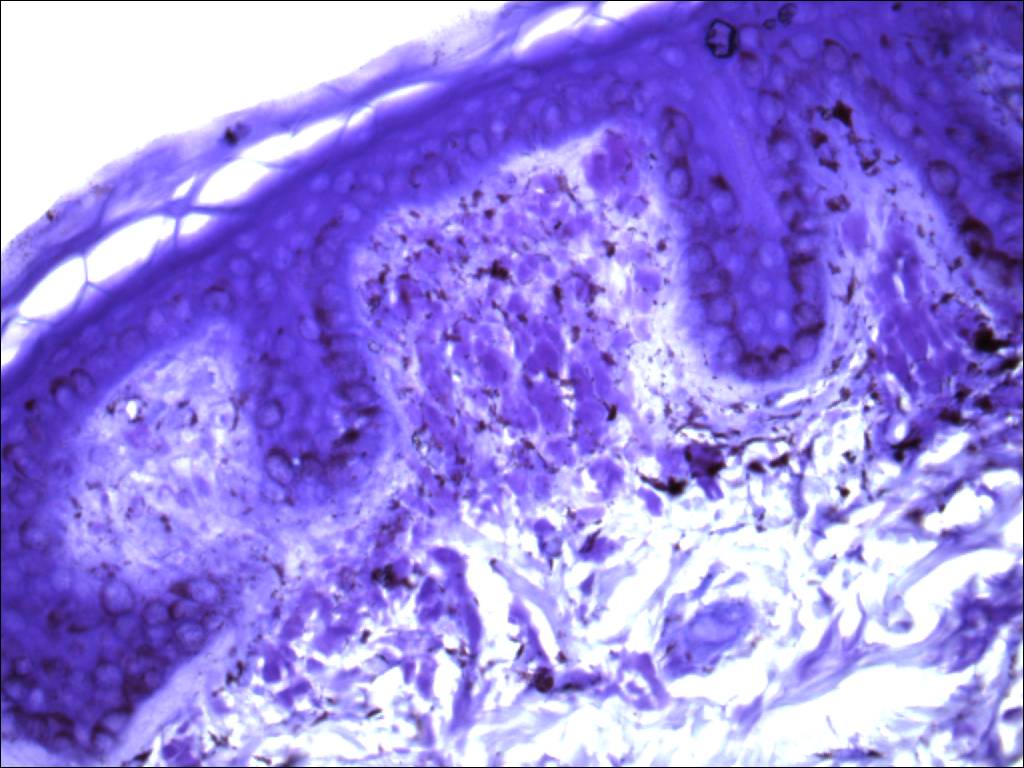
| Figure 9: The globules in Fig. 8 are highlighted by Crystal Violet, suggesting an amyloid derivation; Crystal Violet stain, Mag: 400X. |
In both patients punch biopsies from the conchal bowl yielded a pauci-inflammatory specimen with orthohyperkeratosis and acanthosis (Fig. 4), as well as prominent follicular plugging (Fig. 5). Discrete globules were detected immediately beneath the dermo-epidermal junction in the papillary dermis (Fig. 6). No evidence of interface dermatitis was detected. Electron microscopy studies revealed haphazardly interspersed fibrils consistent with amyloid (Fig. 7). A punch biopsy specimen from the back showed subtle globules with an increased number of mononuclear cells (Fig. 8). These globules were prominently highlighted by a crystal violet stain suggesting an amyloid derivation (Fig. 9).
Comment
Amyloidosis is a depositional disorder with diverse etiologies. It affects multiple organ systems, including the skin. The term amyloid was reportedly coined by the famous 19th century pathologist Virchow who attributed its major constituent to carbohydrate accumulation [1]. Subsequent discoveries have shown amyloid to be a heterogeneous substance that can be derived from a variety of proteins, all of which assume a fibrillar configuration containing β-pleated sheets. Amyloid globules can usually be visualized by light microscopy but are enhanced by crystal violet, thioflavin S, or Congo red stains. Under polarized light microscopy, amyloid stained with Congo red assumes apple-green birefringence. On electron microscopy amyloid appears as haphazard and wavy 6-10 nm non-branching filaments.
Systemic amyloidosis involves the deposition of amyloid in multiple tissues. Cutaneous manifestations of systemic amyloidosis are observed mainly in individuals with a plasma cell dyscrasia, often multiple myeloma. In these instances deposited amyloid derives from immunoglobulin light chains. Cutaneous amyloidosis is associated sporadically with a myriad of inflammatory disorders. Rarely, it is reported to occur as an inherited familial condition [2].
Primary localized cutaneous amyloidosis is, by definition, amyloid deposition limited to the skin and not associated with underlying systemic illness. The two major forms of primary localized cutaneous amyloidosis are lichen amyloidosis and macular amyloidosis. In these conditions, deposited amyloid is keratinocyte derived. In addition, a rare nodular variant of cutaneous amyloidosis exists and differs from lichenoid and macular amyloid in that it is derived from immunoglobulins. The majority of cases of nodular amyloidosis are unassociated with underlying hematological malignancy [3]. In addition to these three forms, cutaneous amyloidosis can also be an incidental histopathologic finding in various neoplasms.
Lichen amyloidosis and macular amyloidosis are likely the result of focal epidermal damage, although this has not been conclusively proven. Histopathologically, these two entities appear to be quite similar and occur as amorphous pink globules in the papillary dermis. They are differentiated by the fact that lichen amyloidosis has more prominent epidermal changes, such as acanthosis and hypergranulosis. Clinically, lichen amyloidosis consists of discrete shiny pruritic papules that may coalesce to form plaques. Lichen amyloidosis occurs primarily on the shins, although other mainly acral sites may be involved. It is thought to be more common in the Asian population. Macular amyloidosis is more subtle in appearance, manifesting as brown macules or papules that coalesce into irregularly pigmented patches or plaques, which may or may not be pruritic, and develop most often on the interscapular back.
In 1983 four cases of smooth papules on the aural conchae were reported by Sanchez [4]. This is likely the first documented finding of lichen amyloidosis in this location, although based on his immunostaining profile they were originally interpreted as being collagenous in nature. These patients were all healthy middle-aged women ages 32-54 who had had their condition for 1-3 years. In 1987, Hicks [5] presented four additional cases of papules on the concha of the ear, which appeared clinically and histologically identical to those previously reported by Sanchez. Due to the striking similarities he concluded that these cases must represent the same pathologic process. Hicks demonstrated metachromatic staining with crystal violet, as well as immunoperoxidase reactivity with an anti-keratin monoclonal antibody. Electron microscopy showed straight, non-branching intermediate filaments densely woven into bundles, which are highly typical for amyloid.
Bakos [6] described a case of papules of the ear that stained positive with Congo Red and were associated with widespread truncal primary cutaneous amyloidosis. Another similar report of biphasic amyloidosis by Barnadas [7] involving the auricular canal not only documented Congo Red positivity but also positive staining with anti-keratin antibodies. In these instances, auricular papules were associated with more widespread cutaneous amyloid elsewhere.
In all, at least a dozen cases of lichen amyloidosis of the auricular concha have been reported in the English literature with additional reports existing in French [8], Spanish [9, 10], and Portuguese [11].
There are several case reports of cutaneous amyloidosis of the auricle occurring in the setting of systemic amyloidosis [12, 13, 14]. Head and neck involvement in systemic amyloid is common. These cases differ from lichen amyloidosis in that the lesions tend to be plaque-like or nodular and are derived from immunoglobulin light chains. In several of these cases infiltrative amyloid deposits became so large as to ultimately lead to hearing difficulties.
The exact relationship between macular and lichenoid amyloidosis is unknown. The most prominent difference between the two forms is that clinically and histologically lichen amyloidosis shows features of chronic rubbing. Not surprisingly, the site predilection of lichen amyloidosis corresponds to areas of the body that are prone to rubbing, whereas the site predilection of macular amyloidosis corresponds to areas of the body that are relatively inaccessible.
In the largest study to date of primary cutaneous amyloidosis, coexistence of lichen and macular amyloidosis in the same patient, termed biphasic amyloidosis, was found in 25 percent of nearly 800 patients [2]. The high prevalence of biphasic amyloidosis supports the notion that lichen amyloidosis and macular amyloidosis are likely different manifestations of the same underlying pathologic process. Other authors have proposed that lichen amyloidosis and macular amyloidosis lie along the same spectrum, and that intermediate forms exist [15]. Analogous to hyperkeratotic lichen planus seen on the shins, lichen amyloidosis can be thought of as hyperkeratotic primary cutaneous amyloidosis. The two cases of lichen amyloidosis of the ear presented here add to the growing number of cases reported at this anatomic site, which is likely the result of ease of accessibility and propensity for rubbing. No cases of macular amyloidosis of the ear have been reported.
The auricular concha is a recognized although unusual site for lichen amyloidosis, and here two additional cases are reported. Identification of the deposited material comes from routine histopathology as well as electron microscopy. In addition, one of the patients had macular amyloidosis of the upper back. The finding of the auricular concha as a site involved in biphasic amyloidosis is of interest, and further supports the theory of lichen and macular amyloidosis as falling on differing ends of the same disease spectrum.
Acknowledgments: The author would like to acknowledge Patrick Creehan MD for bringing patient #2 to his attention and Peter Lynch MD for his helpful comments.
References
1. Picken MM. The changing concepts of amyloid. Arch Pathol Lab Med. 2001 Jan;125(1): 38-43. PubMed.2. Wang WJ, Chang YT, Haung CY, Lee DD. Clinical and histopathological characteristics of primary cutaneous amyloidosis in 794 Chinese patients. Zhonghua Yi Xue Za Zhi (Taipei). 2001 Feb;64(2): 101-7. PubMed.
3. Woollons A, Black MM. Nodular localized primary cutaneous amyloidosis: a long-term follow-up study." Br J Dermatol. 2001 Jul;145(1):105-9. PubMed.
4. Sanchez JL. Collagenous papules on the aural conchae. Am J Dermatopathol. 1983 Jun;5(3): 231-3. PubMed.
5. Hicks BC, Weber PJ, Hashimoto K, Ito K, Koreman DM. Primary cutaneous amyloidosis of the auricular concha. J Am Acad Dermatol. 1988 Jan;18(1 Pt 1): 19-25. PubMed.
6. Bakos L, Weissbluth ML, Pires AK, Muller LF. Primary amyloidosis of the concha. J Am Acad Dermatol. 1989 Mar;20(3): 524-5. PubMed.
7. Barnadas MA, Perez M, Esquius J, Curell R, de Moragas JM. Papules in the auricular concha: lichen amyloidosis in a case of biphasic amyloidosis. Dermatologica. 1990;181(2): 149-51. PubMed.
8. Dupre A, Lassere J, Bonafe JL, Viraben R, Gorguet B.[Collagenous papules of the external ear. Micropapular hyalinosis of the external ear with transepithelial elimination. Relation to primary localized cutaneous amyloidosis] Ann Dermatol Venereol. 1984;111(10): 913-7. PubMed.
9. Mascaró JM. Liquen amiloide del pabellón auricular (case 11). Book of reports VII Reunión Internacional de Dermatología de Barcelona: p26. 1982
10. Echevarria De Martinez, J., F. Nanita de Esteve. Liquen amiloide de pabellon auricular, reporte de ocho casos." Rev Domin Dermatol. 1980 14: 59-63.
11. Weissbluth, M. L. , A. Pires, et al. (1987). "Lichen amilóide com lesóes auriculares." An Bras Dermatol 62: 49-52.
12. Noojin RO, Arrington TS. Unusual cutaneous findings in primary systemic amyloidosis. Arch Dermatol. 1965 Aug;92(2): 157-9. PubMed.
13. El-Sayed, I, Busaba NY, Faquin WC. Otologic manifestations of amyloidosis." Otol Neurotol. 2002 Mar;23(2): 158-9. PubMed.
14. Ambrosone L, Mansi L, Salvatore T, Marino F, Orabona P, Rambaldi A, Rambaldi PF, Rambaldi M. An unusual case of primary systemic amyloidosis. J Eur Acad Dermatol Venereol. 1998 Jan;10(1):53-7. PubMed.
15. Kibbi AG, Rubeiz NG, Zaynoun ST, Kurban AK. Primary localized cutaneous amyloidosis. Int J Dermatol. 1992 Feb;31(2): 95-8. PubMed.
© 2006 Dermatology Online Journal