Effectiveness of bosentan in the treatment of ischemic lesions in a case of thromboangiitis obliterans (Buerger disease): A case report
Published Web Location
https://doi.org/10.5070/D374c2h12cMain Content
Effectiveness of bosentan in the treatment of ischemic lesions in a case of thromboangiitis obliterans (Buerger disease):
A case report
Ángel Palomo-Arellano MD, Iván Cervigón-González, Luis Miguel Torres-Iglesias
Dermatology Online Journal 17 (7): 4
Servicio de Dermatología, Hospital General Ntra. Sra. del Prado, Toledo, Spain. apalomoa@gmail.comAbstract
Buerger disease or thromboangiitis obliterans (TAO) is a thrombotic occlusive, non-atherosclerotic segmental inflammatory disease that affects the small and medium-sized arteries and veins in the extremities of the limbs, frequently requiring amputation. Cessation of tobacco use is the only known effective treatment, though preliminary results from the use of pharmacological therapy implicated in pathogenesis of TAO have demonstrated noticeable clinical improvement of patients. We report the case of a 35-year-old woman with active TAO, refractory to smoking cessation and conventional therapy, who exhibited a favorable clinical response to treatment with bosentan, an oral dual endothelin receptor antagonist, administered on a compassionate-use basis. Six months after starting bosentan therapy, the pain and trophic lesions in the patient's toes had completely disappeared. Bosentan was well tolerated, without any observed adverse reaction. The findings of this case report suggest that bosentan may be considered a therapeutic option for patients with active disease, despite quitting smoking, or for those who fail in absolute abstention from smoking.
Introduction
Buerger disease or thromboangiitis obliterans (TAO) involves segmental vasculitis that affects small and medium sized arteries, veins, and nerves in the upper and lower extremities of the limbs [1]. It usually affects young people from Asia and Eastern Europe and is associated with high tobacco consumption [1].
It is clinically characterized by coldness, intermittent claudication, pain, Raynaud phenomenon, and distal ischemic ulcers that can develop into necrosis and gangrene [1], often requiring amputation.
The only treatment that has been shown to be effective is complete abstention from smoking. In spite of this, the disease progresses in up to 30 percent of cases and finally results in multiple limb amputations, with the consequent increased morbidity and reduction in the patient's quality of life [1].
Vasodilators, antiplatelet agents, anticoagulants, and corticosteroids appear to be of no use [2]. Prostaglandin analogues are beneficial when administered intravenously [3], although no better than placebo on oral administration [4]. Sympathectomy may alleviate the pain and improve superficial ulcers, but it does not prevent or reduce the number of amputations [2]. Surgical revascularisation is not usually feasible because of the diffuse and segmental character of the vasculitis [2]. Omental autografts could be effective in selected patients [5].
In two randomized multicenter placebo-controlled clinical trials, RAPIDS-1 (Randomized Placebo-controlled Investigation of Digital ulcers in Scleroderma) and RAPIDS-2 (Randomized, double blind, Placebo-controlled study with bosentan on healing and prevention of Ischemic Digital ulcers in patients with systemic Sclerosis) [6, 7], bosentan, an orally available dual endothelin-1 (ET-1) receptor antagonist, has confirmed efficacy with a favorable safety profile for the treatment of ischemic digital ulcers (DUs) in scleroderma patients. Bosentan also received approval for a new indication in patients with systemic sclerosis (SSc) and active DUs disease. This treatment has also shown beneficial effects for Raynaud disease in patients with SSc [8, 9].
Bosentan can exert a selective vasodilatory effect on the vascular bed in patients affected by TAO, comparable to the effects observed in connective tissue diseases such as scleroderma with the added complication of digital ulcers. The pathophysiology of the disease is still unknown and various factors have been proposed to be involved in its pathogenesis, one of which is endothelin-1 with its known potent vasoconstrictive effect. Bosentan has recently been used as a method of treatment because of its endothelin receptor antagonism and has shown very good results in improving vascular permeability in digital ischemic ulcers in TAO patients [10, 11].
The present report describes the clinical history of a female patient with active TAO, refractory to smoking cessation and conventional therapy; she achieved a favorable clinical response to treatment with bosentan.
Case report
The present clinical report describes the case history of a 35-year-old from Bulgaria, who had been a smoker of more than 20 cigarettes a day since adolescence, with a 5 year history of disease progression characterized by paleness and coldness in both feet and episodes of pain in the soles of her feet while walking.
 |  |
| Figure 1 | Figure 2 |
|---|---|
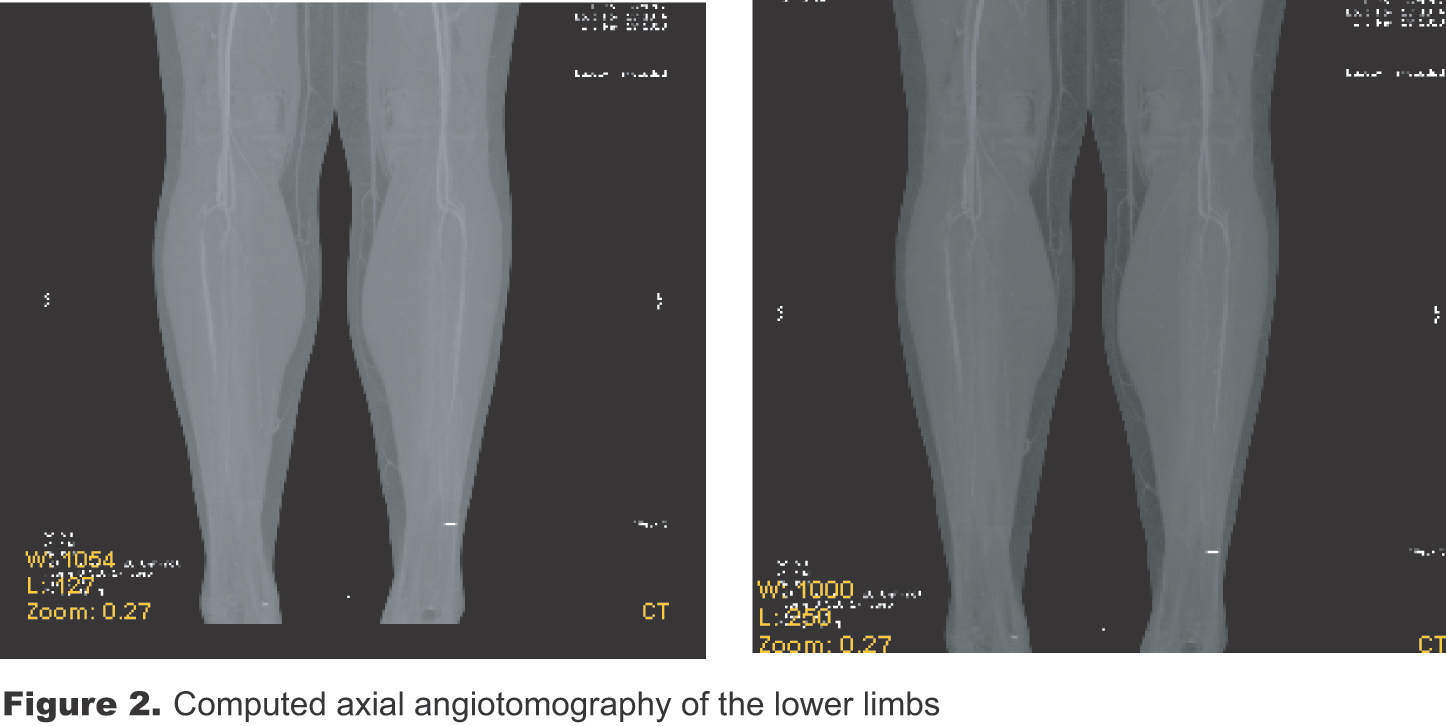
| Figure 1. Ischemic and ulceronecrotic lesions of the soft tissue before treatment with bosentan Figure 2. Computed axial angiotomography of the lower limbs | |
The patient attended the dermatology department because, over the last 12 months, the profile had worsened progressively such that she had pain at rest that was resistant to NSAIDs. She presented with ischemic skin ulcerations on her toes with significant exudation and alterations in the nail plate. On physical examination, paleness, and coldness of the lower limbs, obvious reduction of the pedal pulses, and ulceronecrotic areas of the distal part of the first three toes of both feet were detected (Figure 1). A computed axial angiotomography of the lower limbs revealed a bilateral loss of definition of the infrapopliteal arteries without atheromas (Figure 2). The patient was also referred for full blood workup including acute phase reactants, antinuclear antibodies, rheumatoid factor, and anti-neutrophil cytoplasmic antibodies, which were found to be normal or negative.
Based on the suspected clinical TAO, the patient was told to discontinue tobacco use completely and was prescribed conventional treatment with antiplatelet agents and vasodilators. After one month of conventional treatment and absolute cessation of tobacco use, clinical worsening was observed in the patient. The lesions continued to progress and the pain became so intense that it required a potent treatment with opiate analgesics.
Because of the poor prognosis and the severe pain experienced by the patient, it was therefore decided to initiate bosentan therapy as compassionate treatment, with the intention of accelerating healing of the existing distal cutaneous lesions and to prevent the appearance of new ischemic ulcers.
 |
| Figure 3 |
|---|
| Figure 3. Clinical improvement of trophic lesions after treatment with bosentan |
Written informed consent was obtained from the patient in accordance with regulatory requirements, GCP/ICH, and the Declaration of Helsinki. The patient then began treatment with oral bosentan at an initial dose of 62.5 mg every 12 hours, increasing to a maintenance dose of 125 mg orally twice a day in the fifth week, after first checking that there were no alterations in transaminase levels. After 6 months of therapy, during which time there were no adverse effects clinically or on blood testing to bosentan treatment, the pain completely disappeared and the trophic lesions and ulcers remitted entirely. A control angiotomography showed normal permeability of the infrapopliteal arteries. No new distal cutaneous lesions appeared (Figure 3). It was therefore decided to discontinue medication with bosentan while maintaining the abstention from smoking.
Bosentan was well tolerated, without any adverse reaction observed or biochemical abnormalities detected during the 6 months of bosentan treatment and 9 months of follow-up.
Discussion
Endothelin-1 (ET-1) is a potent vasoconstrictor and pro-inflammatory cytokine that stimulates fibrosis and cell proliferation [12]. ET-1 is mainly secreted by endothelial cells and acts by bonding to the specific receptors (ETA and ETB) present in vascular smooth muscle and the endothelial and epithelial cells of blood vessels [12]. High levels of ET-1 are involved in the pathogenesis of various vascular and connective tissue diseases such as pulmonary hypertension and SSc [13].
Buerger disease appears to involve endothelial cell dysfunction, which leads to an increase in the local synthesis of ET-1. Elevated levels of antibodies to endothelial cells [14] and ET-1 have been detected in patients with TAO. In addition, the plasma concentration of ET-1 correlates with the severity of the vasculitis [15]. Furthermore, impaired endothelium-dependent vaso-relaxation has been observed, whereas the vasodilation mechanisms that do not depend on the endothelium do not appear to be altered [16].
Bosentan is a dual endothelin receptor antagonist with a vasodilating effect (without reflex stimulation of the sympathetic system) and anti-inflammatory, anti-fibrotic, and anti-hypertrophic properties [17]. It is administered orally and has been proven effective in the treatment of pulmonary hypertension, Raynaud phenomenon, and the DUs of patients with SSc [17]. Clinical trials, which included 677 patients, as well as post-marketing surveillance studies, have confirmed that it is a drug with a good safety profile and few side effects (transaminase elevation, which is reversible on reducing or suspending the medication, rhinopharyngitis, facial flushing, swelling of the legs, arterial hypotension, and palpitations) [17, 18].
Systemic sclerosis, a disease in which bosentan has demonstrated its beneficial effect [6, 7], has important clinical (Raynaud phenomenon and ischemic ulcers) and pathogenic similarities (endothelial cell antibodies, increased endothelin levels, and altered vasodilation) to TAO. This, combined with the lack of significant results in the treatment of Buerger disease from other treatment methods, make bosentan a therapeutic option to consider in patients who do not improve on smoking cessation, or who do not manage to give it up completely.
The patient reported about tobacco consumption and no medical diagnostic test was used to confirm the absolute cessation of smoking, which represents a limitation of the present clinical report.
Although there are very few patients with TAO treated with bosentan [10, 11], all of them have shown considerable improvement with few side effects. Nevertheless, rigorous clinical trials with a suitable number of patients are still required to support the use of bosentan in Buerger disease. The findings of this case report have demonstrated that treatment with bosentan has achieved excellent clinical and functional improvement and complete resolution of ischemic cutaneous lesions, avoiding amputation of the affected limbs. The remission of ischemic cutaneous lesions remained so over a follow up period of about 9 months after finishing bosentan treatment.
The therapeutic approach to thromboangiitis obliterans is complex. In spite of smoking cessation and use of vasodilators and anticoagulants, the disease may remain active and lead to distal ischemia which commonly requires amputation of the affected limbs. The administration of an orally available dual endothelin receptor antagonist (bosentan) has recently been used with great efficacy in the treatment of this disease.
In conclusion, the effective use of bosentan for the treatment of distal cutaneous lesions demonstrated in this clinical case and other isolated cases of patients with TAO, suggests that bosentan should be considered as a future therapeutic option in patients that do not improve following cessation of smoking tobacco or who fail in absolute abstention from smoking. Further investigations are warranted to examine the effects of bosentan in the management of TAO patients. Specifically, randomized controlled clinical studies are required to confirm the usefulness of bosentan as a therapeutic option in the treatment of Buerger disease.
Acknowledgments: The authors thank to Lola Montilla from Trial Form Support, Spain, for her contribution in the preparation of this manuscript.
References
1. Olin JW. Thromboangiitis obliterans (Buerger’s disease). N Engl Med. 2000 Sep 21;343(12):864-9. [PubMed]2. Jaff MR. Thromboangiitis Obliterans (Buerger’s disease). Current Treat Options Cardiovasc Med. 2000 Jun;2(3):205-212. [PubMed]
3. Fiessinger JN, Schäfer M. Trial of iloprost versus aspirin treatment for critical limb ischaemia of thromboangiitis obliterans. The TAO Study. Lancet. 1990 Mar 10;335(8689):555-7. [PubMed]
4. The European TAO Study Group. Oral iloprost in the treatment of Thromboangiitis obliterans (Buerger’s disease): a double-blind, randomized, placebo-controlled trial. Eur J Vasc Endovasc Surg. 1998 Apr;15(4):300-7. [PubMed]
5. Agarwal VK. Long-term results of omental transplantation in chronic occlusive arterial diesese (Buerger’s disease) and retinal avascular disease (retinitis pigmentosa). Int Surg. 2007 May-Jun;92(3):174-83. [PubMed]
6. Korn JH, Mayes M, Matucci Cerinic M, Rainisio M, Pope J, Hachulla E, Rich E, Carpentier P, Molitor J, Seibold JR, Hsu V, Guillevin L, Chatterjee S, Peter HH, Coppock J, Herrick A, Merkel PA, Simms R, Denton CP, Furst D, Nguyen N, Gaitonde M, Black C. Digital ulcers in systemic sclerosis: prevention by treatment with bosentan, an oral endothelin receptor antagonist. Arthritis Rheum 2004 Dec;50(12):3985-93. [PubMed]
7. Matucci-Cerinic M, Denton CP, Furst DE, Mayes MD, Hsu VM, Carpentier P, Wigley FM, Black CM, Fessler BJ, Merkel PA, Pope JE, Sweiss NJ, Doyle MK, Hellmich B, Medsger TA Jr, Morganti A, Kramer F, Korn JH, Seibold JR. Bosentan treatment of digital ulcers related to systemic sclerosis: results from the RAPIDS-2 randomised, double-blind, placebo-controlled trial. Ann Rheum Dis. 2011 Jan;70(1):32-8. Epub 2010 Aug 30. [PubMed]
8. Ramos-Casals M, Brito-Zerón P, Nardi N, Claver G, Risco G, Parraga FD, Fernandez S, Julià M, Font J. Successful treatment of severe Raynaud's phenomenon with bosentan in four patients with systemic sclerosis. Rheumatology (Oxford). 2004 Nov;43(11):1454-6. [PubMed]
9. Alegre-Sancho JJ, Fernandez-Llanio N, Hortal-Alonso R, et al. Longterm efficacy and safety of bosentan in the treatment of ischemic digital ulcers due to severe Raynaud’s phenomenon in patients with systemic sclerosis. Proceedings of the Annual European Congress of Rheumatology (EULAR); 2005.
10. De Haro J, Florez A, Fernández JL, et al. Treatment of Buerger disease (thromboangiitis obliterans) with bosentan: a case report. BMJ Case Reports. 2009; 1-3.
11. Todoli Parra JA, Hernández MM, Arrébola López MA. Efficacy of Bosentan in digital ischemic ulcers. Ann Vasc Surg. 2010 Jul; 24(5):690.e1-4. [PubMed]
12. Rubin LJ, Roux S. Bosentan: a dual endothelin receptor antagonist. Expert Opin Investig Drugs. 2002 Jul;11(7):991-1002. [PubMed]
13. Mayes MD. Endothelin and endothelin receptor antagonists in systemic rheumatic disease. Arthritis Rheum. 2003 May; 48(5):1190-9. [PubMed]
14. Eichhorn J, Sima D, Lindschau C, Turowski A, Schmidt H, Schneider W, Haller H, Luft FC. Antiendothelial cell antibodies in thromboangiitis obliterans. Am J Med Sci. 1998 Jan; 315(1):17-23. [PubMed]
15. Czarnacki M, Gacka M, Adamiec R. [A role of endothelin 1 in the pathogenesis of thromboangiitis obliterans (initital news)]. Przegl Lek. 2004;61(12):1346-50. [PubMed]
16. Makita S, Nakamura M, Murakami H, Komoda K, Kawazoe K, Hiramori K. Impaired endothelium-dependent vasorelaxation in peripheral vasculature or patients with thromboangiitis obliterans (Buerger’s disease). Circulation. 1996 Nov 1;94(9 Suppl):II211-5. [PubMed
17. TRACLEER® (bosentan) (Actelion Pharmaceuticals). Summary of product characteristics. Accessed via http://emc.medicines.org.uk, May 2010.
18. Humbert M, Segal ES, Kiely DG, Carlsen J, Schwierin B, Hoeper MM. Results of European post-marketing surveillance of bosentan in pulmonary hypertension. Eur Respir J 2007 Aug;30(2):338-44. Epub 2007 May 15. [PubMed]
© 2011 Dermatology Online Journal