Sarcoidosis
Published Web Location
https://doi.org/10.5070/D36zs3p50cMain Content
Sarcoidosis
Carolyn Kim MD, and William T Long MD
Dermatology Online Journal 10 (3): 24
From the Ronald O. Perelman Department of Dermatology, New York University
Abstract
A 48-year-old woman with an 8-year history of intermittently pruritic papules on the lower extremities suddenly developed pruritus and generalized spread of the lesions over a 1-month period. The lesions appeared as smooth, flat-topped, violaceous, round papules on all extremities, trunk, and back. A biopsy specimen showed sarcoidosis. Cutaneous sarcoidosis has many morphologic presentations and often mimics other dermatologic diseases. Despite widespread cutaneous involvement, she has no systemic involvement. Treatment options are reviewed.
Clinical synopsis
History.—A 48-year-old woman, originally from Guyana, reported an 8-year history of small, intermittently pruritic bumps on her lower extremities. Approximately 4 months prior to her presentation in clinic, larger, similar-appearing lesions began appearing on her abdomen, arms, and back. The lesions were pruritic and became more numerous as she scratched them. Over a 1-month period, the lesions spread to all parts of her body. She denied pain, tenderness, warmth, fevers, chills, arthralgias, or visual disturbances. She has experienced shortness of breath and wheezing for approximately 2 months. After a biopsy was obtained, prednisone was initiated as treatment, which alleviated the pruritus as well as reduced the number of new lesions. However, she could not tolerate the systemic glucocorticoids, because of severe GERD. Methotrexate at a dose of 15 mg weekly was initiated, and prednisone tapered to 5 mg daily. She underwent a pulmonary evaluation, which showed asthma but no other pulmonary involvement.
Past history includes hypothyroidism, breast cancer treated with radiation and lumpectomy in 2001, GERD, and asthma.
Physical examination.— On all extremities, trunk, and back were numerous homogenous, flesh-colored to slightly violaceous, round and polygonal, flat-topped papules that ranged in size from 2 mm to 5 mm. In several areas, the papules have coalesced along lines of excoriation into linear streaks. Very little scale was present. There was no warmth or tenderness to the lesions. The oral mucosa was normal.

|

|
| Figure 1 | Figure 2 |
|---|
|
| Figure 3 |
|---|
Laboratory data.—A complete blood count with differential analysis, chemistry panel, hepatic panel, and iron studies were normal. The total cholesterol and calculated LDL were mildly elevated at 215 mg/dL and 149 mg/dL, respectively. A chest radiograph and chest computed-tomography scan were normal.
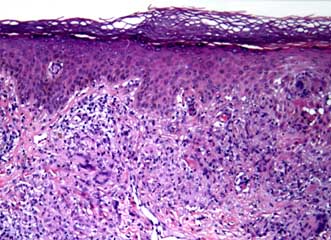
Histopathology.—Epithelioid granulomas and a mild infiltrate of lymphocytes arranged in a bandlike pattern are present in the papillary dermis. The infiltrate obscures the lower portion of a hyperplastic epidermis.
Fite and periodic acid-Schiff stains for microorganisms are negative. No polarizable material is identified.
Diagnosis.—Sarcoidosis.
Comment
Sarcoidosis is a systemic granulomatous disease of unknown etiology. It occurs more frequently in women than in men, with reported ratios as high as 5:1. In two London clinics, sarcoidosis was found to be much more frequent, severe, and extensive in black West Indian, African, Indian, and Pakistani patients than in native white patients. Moreover, in the United States, blacks are affected three to four times more often than are whites. The difference in prevalence among certain populations in varying geographic locations suggests that ethnic susceptibility factors as well as environmental factors contribute to the etiology of sarcoidosis. [1]
Sarcoidosis commonly affects the skin, lungs, lymph nodes, liver, and eyes. Other less frequently affected areas are phalangeal bones, myocardium, central nervous system, kidneys, spleen, and parotid glands. In patients with systemic disease, the skin is involved in 9-37 percent of cases. [2] However, cutaneous lesions are the sole manifestation of sarcoidosis in approximately 25 percent of patients.
Sarcoid is a great imitator of other dermatologic diseases because the cutaneous manifestations are quite variable and have occurred in both local and generalized distributions. Among the numerous reported morphological presentations are papules, micropapules, plaques, nodules, formation in scars, erythroderma, ulcers, and alopecia. Follicular, verrucous, ichthyosiform, hypomelanotic, psoriasiform, and annular lesions have also been described. Moreover, the epidermis can be relatively unaffected in subcutaneous nodules of sarcoid or thin, hypertrophic, discolored, telangiectatic, or scaly. [3,4,5,6,7] Sarcoid lesions are typically asymptomatic, but pruritus is present in approximately 10-15 percent of patients. [2]
Although there are numerous beneficial therapeutic options for sarcoid, little data exists regarding which therapy is best suited for the various cutaneous manifestations. Systemic glucocorticoids are typically beneficial for all patients with sarcoid, although long-term use of high doses is not recommended. Alternatively, intralesional injections of triamcinolone acetonide are suited only for limited skin disease. In cases of extensive skin involvement, chloroquine and hydroxychloroquine have been used, with 75 percent of patients responding either partially or completely. [8,9] Isotretinoin has been beneficial in some patients at doses of 0.5-1.0 mg/kg/day. [10] Methotrexate in doses of 7.5-25 mg weekly has been efficacious in treating sarcoid. However, it has been reported that methotrexate-induced hepatitis occurs in 15 percent of patients with sarcoidosis. [11,12]
Allopurinol has been used to clear refractory and widespread skin lesions. [13] Minocycline and thalidomide have also shown improvement in widespread cutaneous sarcoid lesions. [14,15] Although there are numerous reports of success with various treatments, limited data exists comparing the different treatments, and no controlled studies have been done to date.
References
1. Braverman I. Sarcoidosis. In: Freedberg IM, et al, Eds. Fitzpatrick's Dermatology in General Medicine. McGraw-Hill: New York, 2003:1777.2. Sarcoidosis. Odom RB, et al., Eds. In: Andrews' Diseases of the Skin, 9th edition. W.B. Saunders Company: Philadelphia, 2000:896.
3. Shapiro PE. Noninfectious granulomas. In: Elder D, et al., Eds. Lever's Histopathology of the Skin. Lippincott, Williams and Wilkins: Philadelphia, 1997: 322.
4. Fujii, K, et al. Recurrent follicular and lichenoid papules of sarcoidosis. Eur J Dermatol 2000; 10:303.
5. Glass LA, Apisarnthanarax P. Verrucous sarcoidosis simulating hypertrophic lichen planus. Int J Dermatol 1989; 28:539.
6. Okamoto H, et al. Micropapular sarcoidosis simulating lichen nitidus. Dermatologica 1985; 170:253.
7. Okamoto H. Epidermal changes in cutaneous lesions of sarcoidosis. Am J Dermatopathol 1999; 21:229.
8. Zie JA, et al. Treatment of cutaneous sarcoidosis with chloroquine. Arch Dermatol 1991; 127:1034.
9. Jones E, et al. Hydroxychloroquine is effective therapy for control of cutaneous sarcoidal granulomas. J Am Acad Dermatol 1990; 23:487.
10. Waldinger TP, et al. Treatment of cutaneous sarcoidosis with isotretinoin. Arch Dermatol 1983; 119:1003.
11. Webster GF, et al. Methotrexate therapy in cutaneous sarcoidosis. Ann Intern Med 1989; 111:538.
12. Lower EE, Baughman RP. Prolonged use of methotrexate for sarcoidosis. Arch Intern Med 1995; 155:846.
13. Brechtel B, et al. Allopurinol: a therapeutic alternative for disseminated cutaneous sarcoidosis. Br J Dermatol 1996; 135:307.
14. Bachelez H, et al. The use of tetracyclines for the treatment of sarcoidosis. Arch Dermatol 2001; 137:69.
15. Rousseau L, et al. Cutaneous sarcoidosis successfully treated with low doses of thalidomide. Arch Dermatol 1998; 134:1045.
© 2004 Dermatology Online Journal