Granulomatous rosacea-like demodicidosis
Published Web Location
https://doi.org/10.5070/D36nf1d13jMain Content
Granulomatous rosacea-like demodicidosis
Julia Yu-Yun Lee MD, Chao-Kai Hsu MD
Dermatology Online Journal 13 (4): 9
Department of Dermatology, College of Medicine, National Cheng Kung University, Tainan, Taiwan. yylee@mail.ncku.edu.twAbstract
Demodicidosis may present as pityriasis folliculitis, papulopustular lesions, rosacea-like eruptions, and granulomatous rosacea-like eruptions. We report a case of demodex granuloma presenting with recurrent granulomatous rosacea-like papules on the face in a middle-aged woman. The diagnosis of demodicidosis was made by finding extrafollicular mites in the perifollicular inflammatory infiltrate. The papules resolved after 3 weeks of systemic and topical metronidazole, and low-dose oral prednisolone therapy. In summary, demodex granuloma may be mistaken for granulomatous rosacea-like papules. Correct diagnosis can be facilitated by finding extrafollicular demodex mites in skin biopsy specimens.
Demodex folliculorum is commonly found in the pilosebaceous unit and is the most common ectoparasite in humans. Demodex mites are usually harmless but may induce local inflammation in some individuals when mites are present in excessive numbers or penetrate into the dermis. The role of Demodex folliculorum in various skin disorders has been a subject of many reports for more than half a century and has been reviewed more recently by Baima and Sticherling [1]. Demodicidosis has been classified into pityriasis folliculitis [2], rosacea-like demodicidosis [3] and granulomatous rosacea-like demodiciosis gravis [4]. The clinical manifestation varies from pustular folliculitis [5], papulopustular scalp eruptions [6], blepharitis [7], abscesses [8], and granuloma [9, 10].
Pityriasis folliculorum primarily affects women and manifests a diffuse, faint facial erythema with itching and burning sensations as well as fine follicular plugs and scales imparting a nutmeg-grater, sandpaper-like or frosted appearance. A history of infrequent washing and application of heavy creams and make-up helps to confirm the diagnosis. Rosacea-like demodicidosis manifests erythema, scaling, and papulopustules mimicking common rosacea. However, the scaling in demodicidosis is follicular and the lesions are superficial with small papulovesicles or vesiculopustules. In demodicidosis gravis, the clinical features are similar to granulomatous rosacea with dermal granulomas containing mite remnants phagocytized by foreign-body giant cells and showing central necrosis.
We report a case of demodex granuloma presenting with granulomatous rosacea-like papules on the face, but the diagnosis of demodicidosis was made by finding extrafollicular mites in the perifollicular inflammatory infiltrate.
Report of a case
 |
| Figure 1 |
|---|
| Figure 1. Numerous erythematous, dome-shaped papules are distributed on the face and neck. |
A 48-year-old healthy woman presented with a 6-month history of pruritic skin eruption which responded well to topical corticosteroids but relapsed easily. The patient denied easy flushing. Examination revealed many discrete erythematous papules on the face, neck and anterior chest (Fig. 1). There was no facial telangiectasia. Granulomatous dermatitis or rosacea was suspected. The two indicated figures will appear above this text.
 |  |
| Figure 2 | Figure 3 |
|---|---|
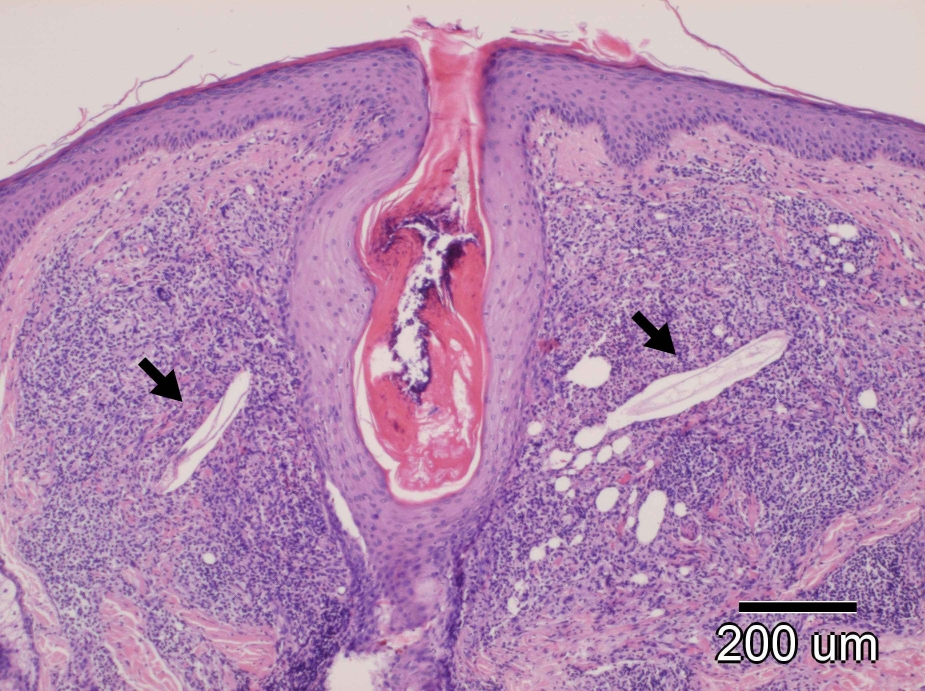
| Figure 2. Biopsy of a papule shows a dense inflammatory infiltrate around a hair follicle with two mites present in the infiltrate
(medium power, hematoxylin and eosin) Figure 3. Close-up view of an extrafollicular mite surrounded by lymphocytes, neutrophils and histiocytes (high power, hematoxylin and eosin) | |
Biopsy of a papule was performed. Histopathologic examination revealed a dense perifollicular mixed inflammatory infiltrate consisting of lymphocytes, neutrophils and histiocytes. Two Demodex mites were found within the perifollicular inflammatory infiltrate (Figs. 2, 3). The papules resolved after 3 weeks of systemic and topical metronidazole, and low-dose of oral prednisolone therapy. There was no recurrence.
Discussion
We described the clinical and pathologic findings of a patient with granulomatous rosacea-like demodicidosis. The diagnosis was established by finding Demodex mites in the perifollicular granulomatous infiltrate. Demodex granuloma should be differentiated from ordinary acne, rosacea, and various papulonodular or granulomatous disorders of the face, including granulomatous rosacea, sarcoidosis, lupus erythematosus, lupus vulgaris, Rosai-Dorfmann's disease, and multicentric reticulohistiocytosis. It is suggested that the diagnosis of demodicidosis could be made by finding five or more of Demodex mites in a single low-power field in a potassium hydroxide preparation [11], or more than 5/cm² in a standardized skin surface biopsy [12]. Demodex mites are more frequently found in rosacea (51%) compared to 28 percent in eczema and 31 percent in discoid lupus erythematosus [13]. Differentiation from rosacea may be difficult when high densities of Demodex mites are present [12, 14]. However, the differential diagnosis will not pose a problem if Demodex mites could be detected in the perifollicular infiltrate, as illustrated in the present case. Hoekzema et al. reported a case of fulminant rosacea-like eruption and reviewed 22 other reported cases of rosacea-like demodicidosis [15]. Intradermal mites have been documented in 15 out of these 23 cases.
It is suggested that the pathogenicity of Demodex mites is a quantitative matter [3]. Several pathogenic mechanisms have been postulated, including blockage of follicles and sebaceous ducts by mites, immune response to mites and their waste products [1].
Various treatments have been used in demodicidosis with variable effects, including topical salicylic acid, metronidazole, crotamiton, lindane, and sublimed sulphur, oral metronidazole, oral ivermectin together with topical permethrin, and oral or topical retinoids [1]. In a patient with demodex abscesses, the infestation was refractory to topical lindane, permthrin, benzoyl benzoate, and oral ivermectin, but resolved rapidly after oral metronidazole 250mg 3 times a day for 2 weeks [8]. In our patient, the facial papules resolved after 3 weeks of systemic and topical metronidazole, and low-dose of oral prednisolone therapy. Metronidazole treatment was also effective in treating three other cases [15, 16, 17].
In summary, we report a case of demodex granuloma presenting with granulomatous rosacea-like papules on the face. Correct diagnosis can be facilitated by finding extrafollicular Demodex mites in skin biopsy specimens.
References
1. Baima B, Sticherling M. Demodicidosis revisited. Act Derm Venereol 2002; 82:3-6.2. Aryes S Jr. Pityriasis folliculorum. Arch Dermatol Syph 1930; 21:19-24.
3. Ayres S Jr. Rosacea-like demodicidosis. Calif Med 1963; 98:228-30.
4. De Dulanto F, Camacho-Martinez. Demodicose 'gravis'. Ann Dermatol Venerol 1979; 106:699-704.
5. Purcell SM, Hayes FJ, Dixon SL. Pustular folliculitis associated with Demodex folliculorum. J Am Acad Dermatol 1986; 15:1159-62.
6. Miskijan S. Demodicidosis (Demodex infestation of the scalp). Arch Dermatol 1951; 63:282-3.
7. Morgan RI, Coston TO. Demodex blepharitis. South Med J 1964; 57:694-99.
8. Schaller M, Sander CA, Plewing G. Demodex abscesses: Clinical and therapeutic challenges. J Am Acad Dermatol 2003; 49:S272-4.
9. Grosshans EM, Kremer M, Maleville J. Demodex folliculorum und die histogenese der granulomatosen Rosacea. Hautarzt 1974; 25:166-77.
10. Ecker RI, Winkelmann RK. Demodex granuloma. Arch Dermatol 1979; 115:343-4.
11. Ayres S Jr. Rosacea and rosacea-like demodicidosis. Int J Dermatol 1987; 26:198-99.
12. Forton F, Seys B, Marchall JL, et al. Demodex folliculorum and topical treatment: acaricidal action evaluated by standardized skin surface biopsy. Br J Dermatol 1998; 138:461-6.
13. Vollmer RT. Demodex-associated folliculitis. Am J Dermatopathol 1996; 18:589-91.
14. Bonnar E, Eustace P, Powell FC. The Demodex mite population in rosacea. J Am Acad Dermatol 1993; 28:443-8.
15. Hoekzema R, Hulsebosch HJ, Bos JD. Demodicidosis or rosacea: what did we treat? Br J Dermatol 1995;133:294-9.
16. Shelley WB, Shelley ED, Burmeister V. Unilateral demodectic rosacea. J Am Acad Dermatol 1989;20:915-7.
17. Lindmaier A, Jusecka W, Lindemayr H. Demodicidosis mimicking granulomatous rosacea and transient acantholytic dermatoses (Grover's disease). Dermatologica 1987;175:200-4.
© 2007 Dermatology Online Journal