Cell Phone Allergic Contact Dermatitis: Case Report and Review
Published Web Location
https://doi.org/10.5070/D36jn7v2xgMain Content
Cell phone allergic contact dermatitis: Case report and review
Anand Rajpara MD, Steven R Feldman MD PhD
Dermatology Online Journal 16 (6): 9
Wake Forest University Department of Dermatology, Winston-Salem, North Carolina. arajpara@gmail.comAbstract
The combination of increased cell phone ownership and unlimited usage plans has led to a situation in which metal cell phone parts may come into contact with the cell phone user’s ear and face for prolonged periods of time. Thus, it is not surprising that recent reports of facial allergic contact dermatitis to cell phone metals have begun to emerge. In this paper we present a case of allergic contact dermatitis to cell phone metal and review all other reports on the subject. We also discuss what the implications of cell phone contact dermatitis are for dermatologists and patients.
Introduction
Around the world the use of cellular phones has dramatically increased over the last decade. Cell phones have become extremely affordable and consumers now have several different cell phone models and wireless providers to choose from. One thing many cell phones have in common is that they contain metal. One thing that all wireless providers have in common is that they offer a popular plan that provides the customer with unlimited cell phone usage at a fixed price. The combination of these two things has led to a situation in which metal cell phone parts may come into contact with the cell phone user’s ear and face for prolonged periods of time. Thus, it is not surprising that recent reports of facial allergic contact dermatitis to cell phone metals have begun to emerge. In this paper we present a case of allergic contact dermatitis to cell phone metal and review all other reports on the subject. We also discuss what the implications of cell phone contact dermatitis are for dermatologists and patients.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|---|
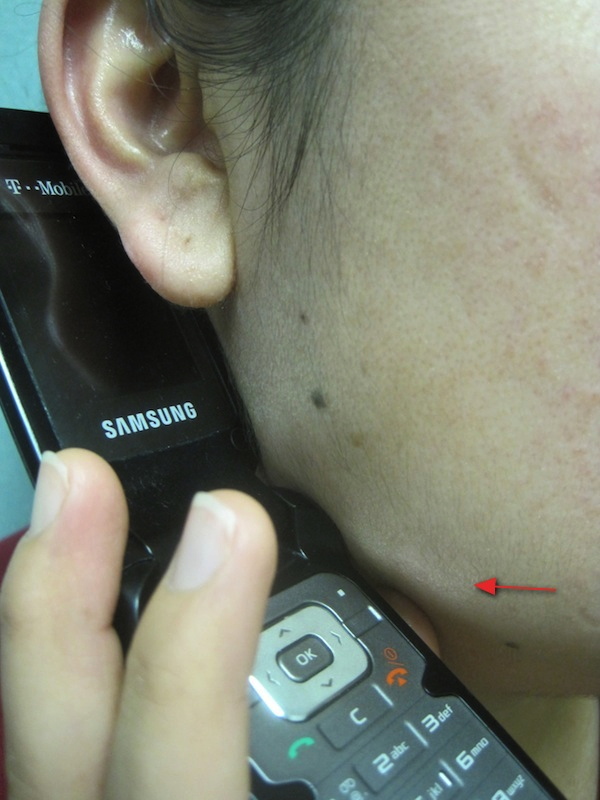
| Figure 1. Patch of dermatitis above patient’s right jaw line Figure 2. Close-up of patch of dermatitis above patient’s right jaw line | |
 |
| Figure 3 |
|---|
| Figure 3. Patient’s metallic cell phone menu button lines up directly with patch of dermatitis above patient’s right jaw line |
A 28-year-old woman presented with an isolated itchy, dry patch on her right cheek. On physical exam there was a patch of dermatitis on her right jaw line that corresponded with the spot where the metallic menu button on her cell phone contacted her skin (Figures 1, 2, and 3). She was clinically diagnosed with allergic contact dermatitis and advised to avoid contact with the metal allergen on her cell phone. During a follow up phone call the patient reported that she achieved marked improvement in her dermatitis by limiting her cell phone use and avoiding direct skin contact with the cell phone when using it. For convenience purposes we suggested to the patient that she try covering the metal parts of her cell phone with a plastic film as an alternative treatment option.
Comments
Cell phone use has increased dramatically over the past 10 years all over the world. Cell phone ownership among teenagers aged 12-17 in the U.S. increased from 33 percent in 2002, to 55 percent in 2006 [1]. In addition, unlimited usage plans may result in cell phone use for prolonged periods of time. Exposure of the ear and facial skin to metal cell phone parts for long time periods has led to the emergence of several reports of contact dermatitis to the metal allergens, nickel sulfate and hexavalent chromium.
Nickel is found in many objects encountered on a daily basis including keys, coins, and paper clips. However, since contact with such objects is generally brief, nickel allergy does not usually develop. The risk of nickel allergy is increased by frequent, prolonged exposure to nickel-containing object, such as occurs with necklaces, watches, and earrings. Nickel is the most common contact allergen and affects up to 17 percent of women and 3 percent of men [2]. Allergic cell phone contact dermatitis in response to nickel was first reported in 2000 in Italy by Pazzaglia et al. [3] and since then, a few other case reports from around the world have emerged (Table 1). The most common cell phone sites containing free nickel include the decorative logos on headsets, menu buttons, and the metal frames around the LCD (liquid crystal display seen) [4]. Thus, cell phone contact dermatitis typically presents as patches of dermatitis involving areas of the unilateral ear and/or face that correspond to the metal parts of the cell phone that touch the face.
In 1994 the EU Nickel Directive was created to protect citizens from nickel allergy by prohibiting consumer products that had direct and prolonged contact with the skin and released more than a pre-determined level of free nickel. Since that time two reports have shown that the prevalence of nickel allergic contact dermatitis has decreased in Germany and Denmark [7, 8]. A Danish Study found that 8 of 41 cell phones tested using the dimethylglyoxime test released free nickel; a similar study in Canada revealed 4 of 22 mobile phones tested released excessive nickel [5, 6]. As a result, in 2009 the European Union Nickel Directive expanded its original policy to include cell phones.
Nine cases of cell phone contact dermatitis associated with hexavalent chromium have also been reported by one group in Japan (Table 2) [9, 10]. In 8 of the 9 reported cases patch testing confirmed chromate allergy and ruled out nickel allergy. Just one patient demonstrated allergy to both chromate and nickel. Chromate is not as common a contact allergen as nickel. One study of 3440 patients designed to measure the prevalence of various contact allergens using patch testing found the prevalence of chromate allergy to be 2.8 percent [11]. Chromate is typically found in industrial materials like stainless steel and cement. Unlike nickel, chromate by itself is not a contact allergen and must react with sweat, saliva, or plasma in order to become allergenic [12]. It is hypothesized that during prolonged cell phone use, the chromate from the cell phone reacts with human sweat to become a contact allergen causing contact dermatitis [9].
Treatment for cell phone contact dermatitis includes covering the cell phone with a plastic film [3], using a wireless ear piece, or switching to a different cell phone that does not contain metal on surfaces that contact the skin. In the case of nickel allergy, patients can purchase nickel spot-test kits from their local pharmacy and can easily test phones for free nickel before purchasing or using them. In conclusion, cell phone allergic contact dermatitis is an emerging problem and should be considered in the differential diagnosis for unilateral ear and/or face dermatitis.
References
1. Meyerson B. Schools crack down on cellphones. MSNBC; 2006 (accessed 2010 Apr 7).2. Thyssen J P, Linneberg A, Menné T, Johansen J D. The epidemiology of contact allergy in the general population – prevalence and main findings. Contact Dermatitis 2007: 57: 287–299. [PubMed]
3. Pazzaglia M, Pasquale L, Colombina V, Tosti A. Contact dermatitis from nickel in mobile phone. Contact Dermatitis 2000: 42: 362–363. [PubMed]
4. Bercovitch L, Luo J. Cellphone Contact Dermatitis with Nickel Allergy. CMAJ 2008: 178 (1); 23-24. [PubMed]
5. Thyssen J P, Johansen J D, Zachariae C, Menné T. The outcome of dimethylglyoxime testing in a sample of cell phones in Denmark. Contact Dermatitis 2008: 59: 38–42. [PubMed]
6. Livideanu C, Giordano-Labadie F, Paul C. Cellular phone addiction and allergic contact dermatitis to nickel. Contact Dermatitis 2007: 57: 130–131. [PubMed]
7. Schnuch A, Uter W. Decrease in nickel allergy in Germany and regulatory interventions. Contact Dermatitis 2003: 49: 107–108. [PubMed]
8. Johansen J, Menné T, Christophersen J, Kaaber K, Veien N. Changes in the pattern of sensitization to common contact allergens in Denmark between 1985-86 and 1997-98, with a special view to the effect of preventive strategies. Br J Dermatol 2000: 142: 490–495. [PubMed]
9. Seishima M, Oyama Z, Yamamura M. Cellular phone dermatitis. Arch Dermatol 2002: 138: 272–273. [PubMed]
10. Seishima M, Oyama Z,Makiko O. Cellular phone dermatitis with chromate allergy. Dermatology 2003: 207: 48-50. [PubMed]
11. Marks JG, Belsito DV, DeLeo VA, et al. North American Contact Dermatitis Group patch-test results, 1996-1998. Arch Dermatol. 200;136:272-273. [PubMed]
12. Kanerva L, Aitio A. Dermatotoxological aspects of metallic chromium. Eur J Dermatol. 1997;7:79-84.
© 2010 Dermatology Online Journal