Erythema dyschromicum perstans and vitiligo
Published Web Location
https://doi.org/10.5070/D365k223kzMain Content
Erythema dyschromicum perstans and vitiligo
Narayan S Naik MD
Dermatology Online Journal 9(4): 25
From the Ronald O. Perelman Department of Dermatology, New York University
Abstract
We report an East Indian man with simultaneous lesions of erythema dyschromicum perstans and vitiligo. This report is only the second to present these two pigmentary disorders occurring in the same patient. Although the exact cause of both disorders is unknown, a pathogenetic role for cytotoxic T-cell responses has been hypothesized in each condition.
Clinical summary
History.—A 33-year-old man was seen for a 6-month history of depigmentation involving the lips, trunk, and extremities. The patient presented to Bellevue Hospital Center dermatology clinic in January 2002 with a 20-year history of depigmented patches on his trunk and extremities. In addition, he had noted the development of gray-blue patches on the trunk and arms over the last 6 months. Previously, he had been treated in India with a pill and light exposure for a period of 16 years. The last treatment was more than 5 years ago. The patient denied any cutaneous eruptions preceding either type of color change. He also denied any chemical exposure to the affected areas. The patient was otherwise healthy, and there was no history of similar disorders in other family members. A biopsy was taken from the edge of a gray-blue patch.
Physical examination.—Confluent, gray-blue patches with fine scale were present over the torso and arms. Depigmented patches were present over the anterior legs, upper chest, mid-to-lower back, lips, and dorsal hands. In some areas, superimposed erythema and mottled brown hyperpigmentation were noted. The patches were not hypesthetic. Wood's lamp examination accentuated the depigmented areas but had no effect on the gray-blue patches.

|
|
| Figure 1 | Figure 2 |
|---|
Laboratory data.—None
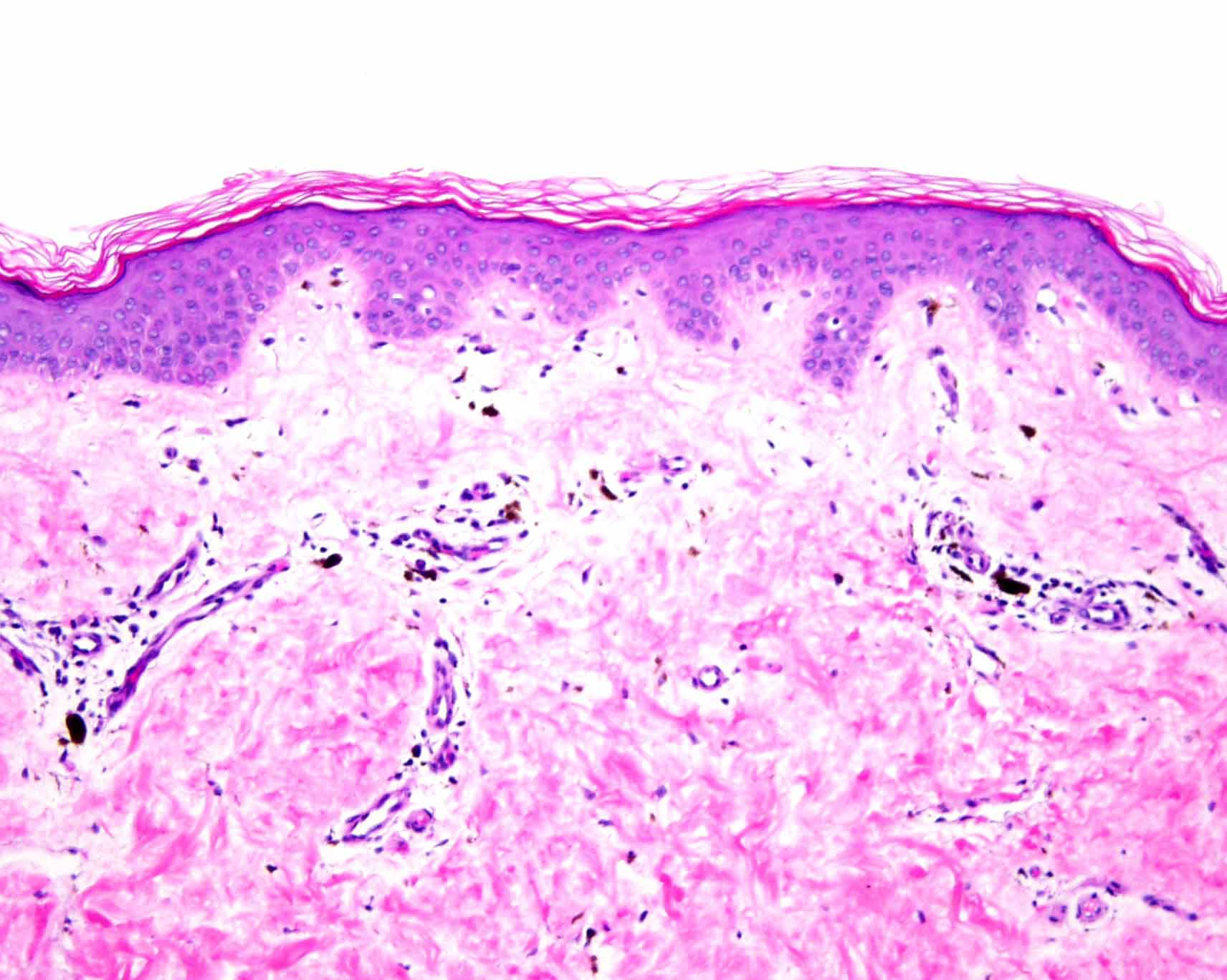
Histopathology.—Hematoxylin-and-eosin stained sections show a sparse, superficial, perivascular infiltrate composed of lymphocytes and macrophages containing melanin. A Fontana-Masson stain shows a normal number of pigmented melanocytes in the basal layer of the epidermis.
Diagnosis.—Erythema dyschromicum perstans and vitiligo.
Comment
Erythema dyschromicum perstans, or ashy dermatosis, is an uncommon, idiopathic, chronic, pigmentary disorder that is characterized by gray, macular, cutaneous discoloration. The eruption coalesces into confluent patches that may assume oval or polycyclic configurations. The sites of predominance are the trunk and proximal portions of the extremities. A palpable erythematous ridge characterizes the lesions' periphery. This raised border usually fades in more advanced lesions. Although the condition may occur at any age, it often begins under age 40. The disorder is more common in Latin Americans and Asians.
Some authors have proposed a relationship between erythema dyschromicum perstans and lichen planus. The diseases have coincided in a number of patients [1, 2]. The disorder has been described as closely resembling two lichen planus variants—lichen planus actinicus and lichen planus pigmentosus[1, 2]. Histologic features such as a superficial lymphoid infiltrate, vacuolar interface change, and pigmentary incontinence also suggest a lichenoid process. Direct immunofluorescence findings of cytoid bodies provide further support for this hypothesis [3].
There is only one previous report of erythema dyschromicum perstans and vitiligo occurring in the same patient [4]. A study evaluating the inflammatory cells in each condition showed a predominance of cytotoxic T-cells and an increase in Langerhans cells in the epidermis of both erythema dyschromicum perstans and early lesions of vitiligo [5].
No single established therapy exists for erythema dyschromicum perstans. However, clofazamine given over several months appears to have benefit in a majority of patients [6]. Although this benefit may result from the uniform skin discoloration produced by the drug, there is also evidence of anti-inflammatory and immunomodulatory effects on this condition [7].
References
1. Berger RS, et al. Erythema dyschromicum perstans and lichen planus: are they related? J Am Acad Dermatol 1989, 21:438.2. Naidorf KF, Cohen SR. Erythema dyschromicum perstans and lichen planus. Arch Dermatol 1982;118:683.
3. Miyagawa S, et al. Erythema dyschromicum perstans: immunopathologic studies. J Am Acad Dermatol 1989; 20:882.
4. Anderson CD, et al. Simultaneously active lesions of vitiligo and erythema dyschromicum perstans. Arch Dermatol 1988; 124: 1258.
5. Gross A, et al. Mononuclear cell subpopulations and infiltrating lymphocytes in erythema dyschromicum perstans and vitiligo. Histol Histopathol 1987; 2: 277.
6. Piquero-Martin J, et al. Clinical trial with clofazamine for treating erythema dyschromicum persans. Int J Dermatol 1989; 28:198.
7. Baranda L, et al. Involvement of cell adhesion and activation molecules in the pathogenesis of erythema dyschromicum perstans (ashy dermatitis): the effect of clofazimine therapy. Arch Dermatol 1997;133:325.
© 2003 Dermatology Online Journal