Explosive nasofacial cryptococosis
Published Web Location
https://doi.org/10.5070/D35zp118s2Main Content
Explosive nasofacial cryptococosis
Paul Persad MD, Rajendrakumar Patel MD, Jeffery Stephens MD, Sandy Francis-Rogers MD, Praveen Talat MD
Dermatology Online Journal 16 (3): 5
Mercer University School of Medicine, Macon, Georgia. paulpersad@yahoo.comAbstract
Cryptococcal skin infection in persons with AIDS has been demonstrated. We describe a patient with nasal and facial infection with cryptococci after traumatic injury with battery acid.
Case presentation
A 60-year-old black male with AIDS and recurrent cryptococcal meningoencephalitis who was noncompliant with antiretroviral therapy, presented with complaints of a headache of 3 days duration that had been progressively worsening. On further questioning the patient stated that he had sustained a facial injury two weeks previous to presentation when an automobile battery accidentally exploded. His facial injuries did not heal and developed into lesions that were most visible on his nose but also apparent on his scalp and neck. Progressively worsening and severe headaches that began three days previously, however, were his primary reason for coming to the Emergency Center.
A diagnosis of HIV-1 infection had been made in 2005. At that time the CD4 lymphocyte count was 50 cells/ml and the viral load was 19,000 RNA copies/ml. Highly active antiretroviral therapy (HAART) was initiated at that time but he was subsequently lost to follow up. During this hospitalization a lumbar puncture demonstrated elevated opening pressure, a positive CSF cryptococcal antigen, and a positive India ink, consistent with crytpococcal meningitis. Serum cryptococcal antigen testing was also positive.
 |
| Figure 1 |
|---|
| Figure 1. Face of patient |
The cutaneous exam revealed multiple scattered crusted lesions on his scalp, face, and neck ranging in size from 1 to 3 cm (Figure 1). Some papules and plaques demonstrated umbilication and ulceration. Plaque confluence was noted on his nose with some extension into the nasal passages. There were no mucosal lesions or palpable lymphadenopathy. No neurological impairment was noted and the plaques and nodules were not painful. Kernig and Brudzinski signs were negative. Cerebrospinal fluid studies, as previously mentioned, confirmed cryptococcal meningitis. Blood cultures remained negative.
 |
| Figure 2 |
|---|
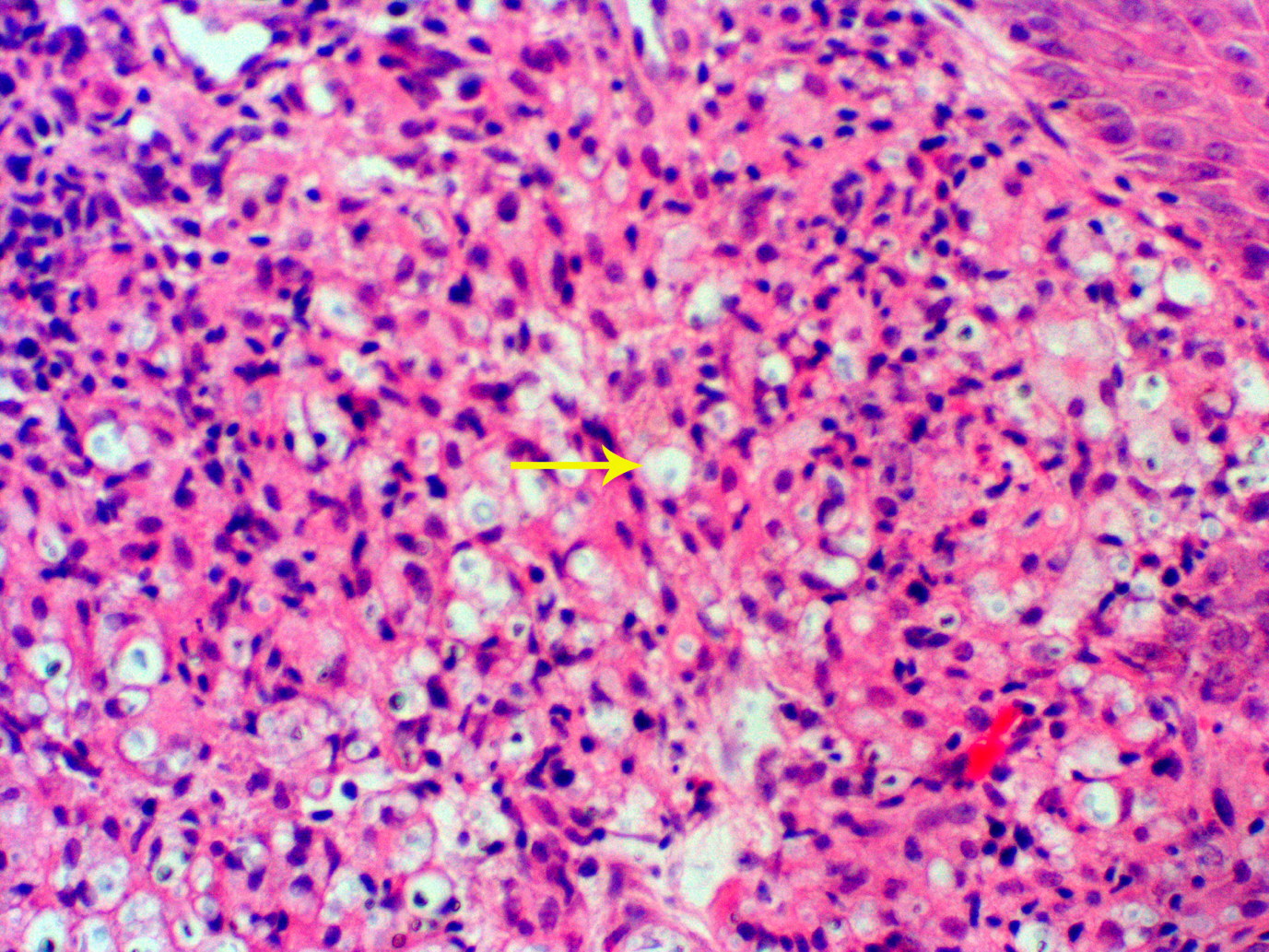
| Figure 2. High power image highlighting the intra-histiocytic yeasts (x20) |
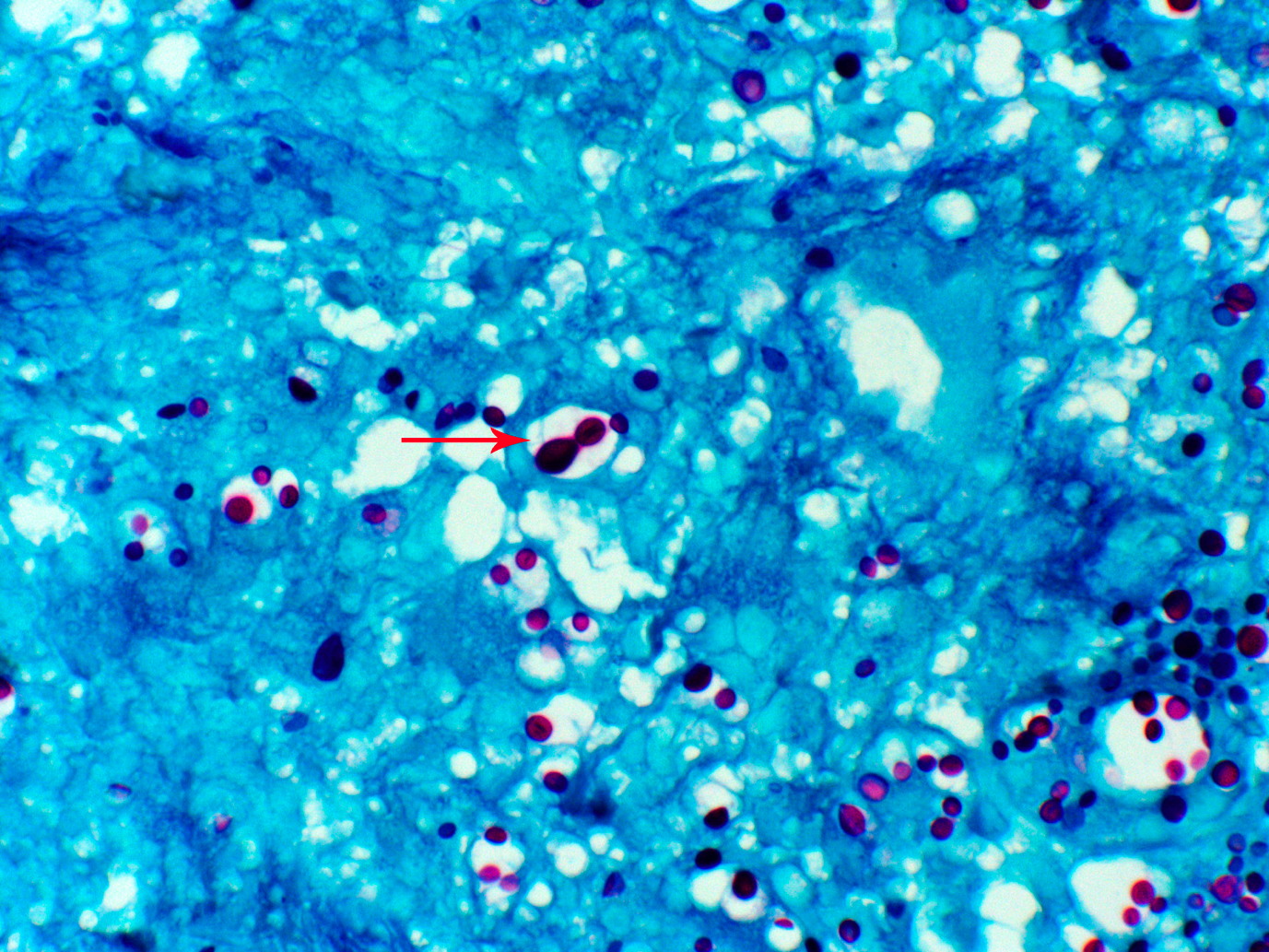
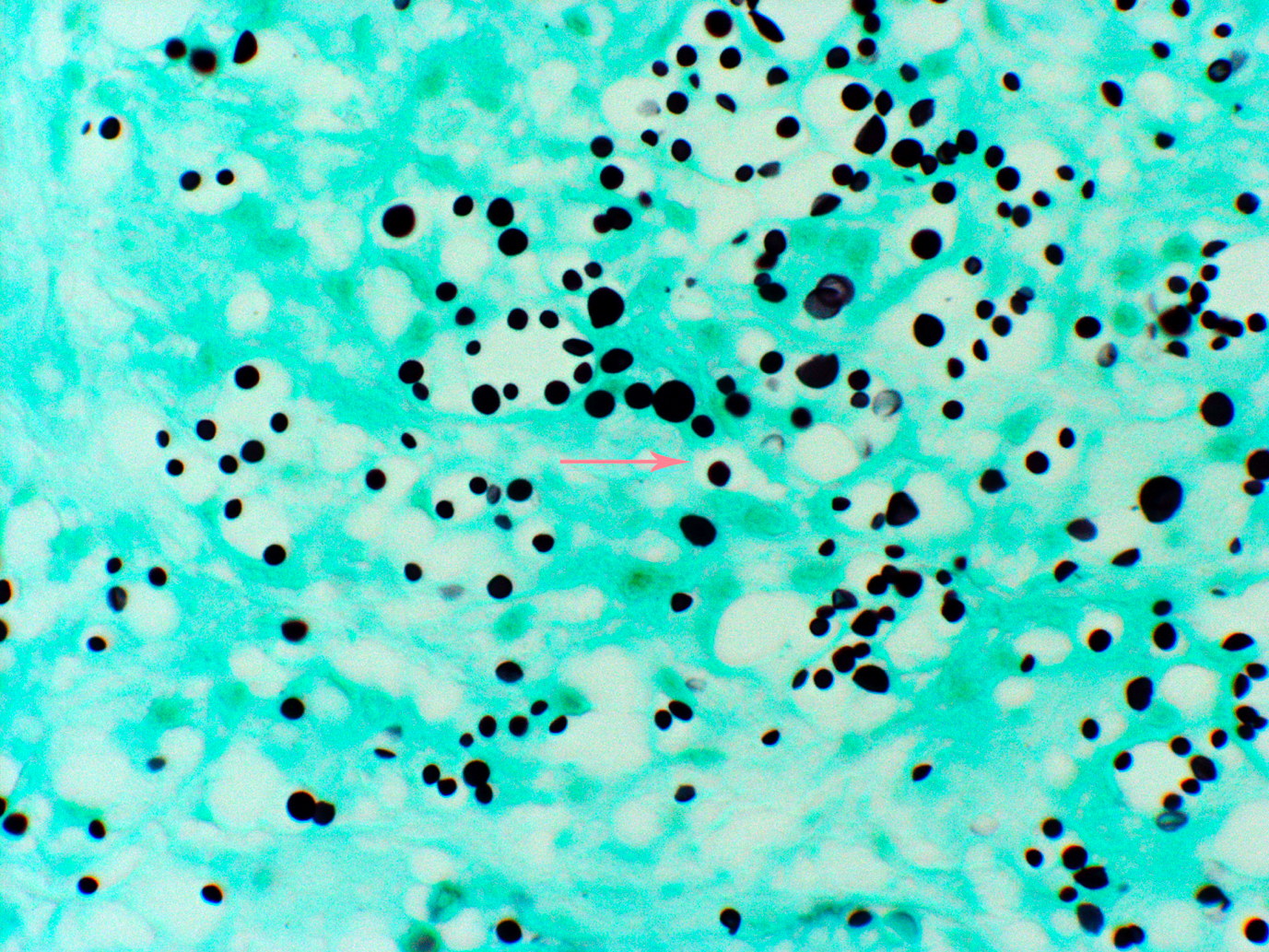
Skin biopsy (Figure 2) of an upper lip papule revealed budding yeast consistent with Cryptococcus infection. Microscopic examination revealed skin with ill-defined granulomatous inflammation predominantly consisting of epithelioid histiocytes, scattered mixed inflammatory cells, and a few giant cells. The overlying epidermis showed active inflammation and pseudoepitheliomatous hyperplasia. Numerous intra-histiocytic, round to oval, narrow-based budding yeasts with large polysaccharide capsules, morphologically consistent with cryptococcus neoformans were noted. Fungal stains were also positive in the specimens (Figures 3 and 4).
 |  |
| Figure 3 | Figure 4 |
|---|---|
| Figure 3. Periodic acid-Schiff positive narrow-based budding yeasts (x40) Figure 4. Gomori methenamine silver positive narrow-based budding yeasts (x40) | |
Our patient’s CNS disease was treated with amphotericin B at 1 mg/kg/day plus flucytosine at 100 mg/kg/day for 2 weeks. This was followed by fluconazole 400 mg per day for 6 weeks, then 200 mg daily indefinitely. His headaches resolved before discharge from the hospital. His facial lesions were modestly improved. Within 2 months the patient was seen again in our HIV clinic with near complete resolution of his facial lesions. Unfortunately, he declined additional photography. Subsequently he was lost to follow up and presumably discontinued his suppressive therapy.
Discussion
Cryptococcus neoformans is a common worldwide opportunistic pathogen [1]. This organism was first identified in peach juice by Sanfelice in 1894 [2]. Busse and Buschke documented the first human case of cryptococcal skin infection in 1895 [3]. Clinical presentations vary from asymptomatic colonization of the airways to disseminated infection of virtually any body part including the central nervous system, bones, skin, and reproductive organs [4]. Skin infection with C. neoformans is the third most common organ affected after the lungs and CNS. The major virulence factor, the polysaccharide capsule [5], is responsible for antiphagocytosis and is the basis for serotyping [6, 7]. The capsule is composed of two large polysaccharides, glucuronoxylomannan, and galactoxylomannan, along with mannoproteins [8]. Capsular interaction with dermal dendritic cells plays a key role in cutaneous immune activation [9]. Furthermore, crytpococcal adaptations for survival against ameoba may further explain its virulence in humans [10]. The polysaccharide capsule has been demonstrated to impair amoebic ability to eliminate this fungus once internalized. In acapsular strains of cryptococci, melanin production protects from intracellular oxidative damage. These mechanisms are thought to contribute to cryptococcal pathogenicity within mammalian macrophages [10]. Viral infections like HIV and HSV have been shown to further impair host monocyte responses to fungal challenge [11].
Cutaneous examination often demonstrates a papule with a soft or ulcerated center that may appear umbilicated. Some lesions are easily mistaken for molluscum contagiousum, Kaposi sarcoma, acne vulgaris, basal cell carcinoma, or squamous cell carcinoma. Other manifestations appear similar to bacterial cellulitis or abscesses [12]. Biopsy and histopathologic confirmation are essential for correct diagnosis, especially in the immunocompromised host. Traumatic inoculaton of the skin with cryptococci has been described [13]. Immunosuppressed hosts may be at heightened risk for disease in this situation [14, 15]. Immune reconstitution inflammatory syndrome in HIV patients treated with HAART is also a known precipitant of cryptococcal skin disease [16]. Non-HIV populations at risk include cancer patients [17] and those on long-term corticosteroids [18]. Furthermore, liver transplant recipients treated with tacrolimus are also at an increased risk of cryptococcal skin infection [19].
Recommended treatment for non-CNS disseminated cryptococcosis in the immunocompromised host includes fluconazole 200-400 mg daily for 3-6 months or itraconazole 200-400 mg daily for 6-12 months [20]. In cases of concomitant CNS disease and cutaneous disease as in our patient, amphotericin B 0.5-1 mg/kg/day plus flucytosine 100 mg/kg/day for 2 weeks followed by fluconazole 400 mg daily for 6 weeks then 200 mg daily for life will treat both the skin and CNS disease [20].
Our case demonstrates that even when given a history of coincident trauma, cyptococcal skin infection can underlie disseminated disease in immunocompromised hosts. Skin biopsies are therefore necessary to evaluate the possibility of dissemination, secondary infections, or concomitant neoplasms in these patients.
References
1. Dharmshale SN, Patil, SA, Gohil A, Chowdhary A, Oberor C. Disseminated cryptococcosis with extensive cutaneous involvement in AIDS. Indian J Med Microbiol. 2006 Jul;24(3):228-30. [PubMed]2. Swinne D. Cryptococcus neoformans and the epidemiology of cryptococcosis. Ann Soc Beig Med Trop. 1979 Sep;59(3): 285-99. [PubMed]
3. Knoke M, Schwesinger G. One hundred years ago: the history of cryptococcosis in Greifswald. Medical mycology in the nineteenth century. 1994 Jul-Aug; 37(7-8):229-33. [PubMed]
4. Calista D, Grosso C. Cutaneous cryptococcosis of the penis. Dermatol Online J. 2008 Jul 15; 14(7):9. [PubMed]
5. Chang YC, Kwong-Chung KJ. Complementation of a capsule-deficient mutation of Cryptococcus neoformans restores its virulence. Mol Cell Biol. 1994 Jul;14(&):4912-9. [PubMed]
6. Dromer F, Geuho E, Ronin O, Dupont B. Serotyping of Cryptococcus neoformans by using a monoclonal antivody specific for capsular polysaccharide. J Clin Microbiol. 1993 Feb;31(2):359-63. [PubMed]
7. Gates MA, Thorkildson P, Kozel TR. Molecular architecture of the Cryptococcus neoformans capsule. Mol Microbiology. 2004 Apr;52(1):13-24. [PubMed]
8. Doering TL. How Sweet it is! Cell Wall Biogenesis and Polysaccharide Capsule Formation in Cryptococcus neoformans. Annu Rev Microbiol. 2009;63:223-47. [PubMed]
9. Buentke E, Scheynius A. Dendritic Cells and fungi. APMIS. 2003 Jul-Aug;111(7-8):789-96. [PubMed]
10. Steenbergen JN, Shuman HA, Casadevall A. Cryptococcus neoformans interactions with amoebae suggest an explanation for its virulence and intracellular pathogenic strategy in macrophages. Proc Natl Acad Sci U S A. 2001 Dec 18;98(26):15245-50. [PubMed]
11. Cermelli C, Orsi CF, Ardizzoni A, Lugi E, Cenacchi V, Cossarizza A, Blasi E. Herpes simplex virus type 1 dysregulates anti-fungal defenses preventing monocyte activation and downregulating toll-like receptor-2. Mircrobiol Immunol. 2008 Dec;52(12):575-84. [PubMed]
12. Anderson DJ, Schmidt C, Goodman J, Pomeroy C. Cryptococcal disease presenting as cellulitis. Clin Infect Dis. 1992 Mar;14(3):666-72. [PubMed]
13. Revenga F, Paricio JF, Merino FJ, Nebreda T, Ramirez T, Martinez AM. Primary cutaneous cryptococcosis in an immunocompetent host: case report and review of the literature. Dermatology. 2002;204(2):145-9. [PubMed]
14. Bauza A, Redondo P, Rubio M. Primary cutaneous cryptococcal cellulitis secondary to insect bite in an immunosupressed patient after liver transplant. Clin Exp Dermatol. 2005 May;30(3);241-3. [PubMed]
15. Hafner C, Linde, HJ, Vogt T, Breindl G, Tintelnot K, Koellner K, landthaler M, Szeimies RM. Primary cutaneous cryptococcosis and secondary antigenemia in a patient with long-term corticosteroid therapy. Infection. 2005 Apr;33(2):86-9. [PubMed]
16. Broom J, Woods M 2nd, Allworth A. Immune reconstitution inflammatory syndrome producing atypical presentations of cryptococcal meningitis: case report and a review of immune reconstitution-associated cryptococcal infections. Scand J Infect Dis. 2006;38(3):219-21. [PubMed]
17. Kontoyiannis DP, Peitsch WK, Reddy BT, Whimbey EE, Han XY, Bodey GP, Rolston KV. Cryptococcosis in patients with cancer. Clin Infect Dis. 2001 Jun 1;32(11):E145-50. Epub 2001 May 4. [PubMed]
18. Moosbrugger EA, Adams BB, Kralovic SM. Cutaneous Cryptococcosis in a patient on corticosteroid therapy for rheumatoid arthritis. Int J Dermatol. 2008 Jun;47(6):630-2. [PubMed]
19. Singh N, Gayowski T, Wagener MM, Marino IR. Clinical spectrum of invasive cryptococcosis in liver transplant recipients tacrolimus. Clin Transplant. 1997 Feb;11(1):66-70. [PubMed]
20. Kaplan JE, Benson C, Holmes KH, Brooks JT, Pau A, Masur H. Guidelines for prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: Recommendations from the CDC, the National Institutes of Health, and the HIV Medicine Association of the Infectious Disease Society of America. MMWR Recomm Rep. Apr 10 2009;58:1-207. [PubMed
© 2010 Dermatology Online Journal