Purpuric drug eruption and alopecia induced by erlotinib
Published Web Location
https://doi.org/10.5070/D35bw35558Main Content
Letter: Purpuric drug eruption and alopecia induced by erlotinib
Taeko Nakamura-Wakatsuki, Toshiyuki Yamamoto
Dermatology Online Journal 18 (5): 16
Department of Dermatology, Fukushima Medical University, Fukushima, JapanAbstract
We herein report a case of diffuse alopecia with pustules on the scalp and purpuric lesions on the lower legs in a Japanese man after treatment with erlotinib. This is a unique case in which rare skin eruptions simultaneously occurred. We discuss herein a combination of skin eruptions as an adverse reaction of epidermal growth factor-receptor (EGF-R) tyrosine kinase inhibitor. It is indispensable to be aware of rare skin reactions when applying molecular targeting therapies.
Introduction
Erlotinib is a novel tyrosine kinase inhibitor targeting the epidermal growth factor receptor (EGF-R), which is used for prior chemotherapy-resistant non-small cell lung cancer. Skin eruption is the most common adverse reaction and an acneiform eruption is most frequently reported. We herein report a rare case of alopecia with pustules on the scalp along with purpuric lesions on the lower legs that occurred after treatment with erlotinib.
Case report
 |  |
| Figure 1a | Figure 1b |
|---|---|
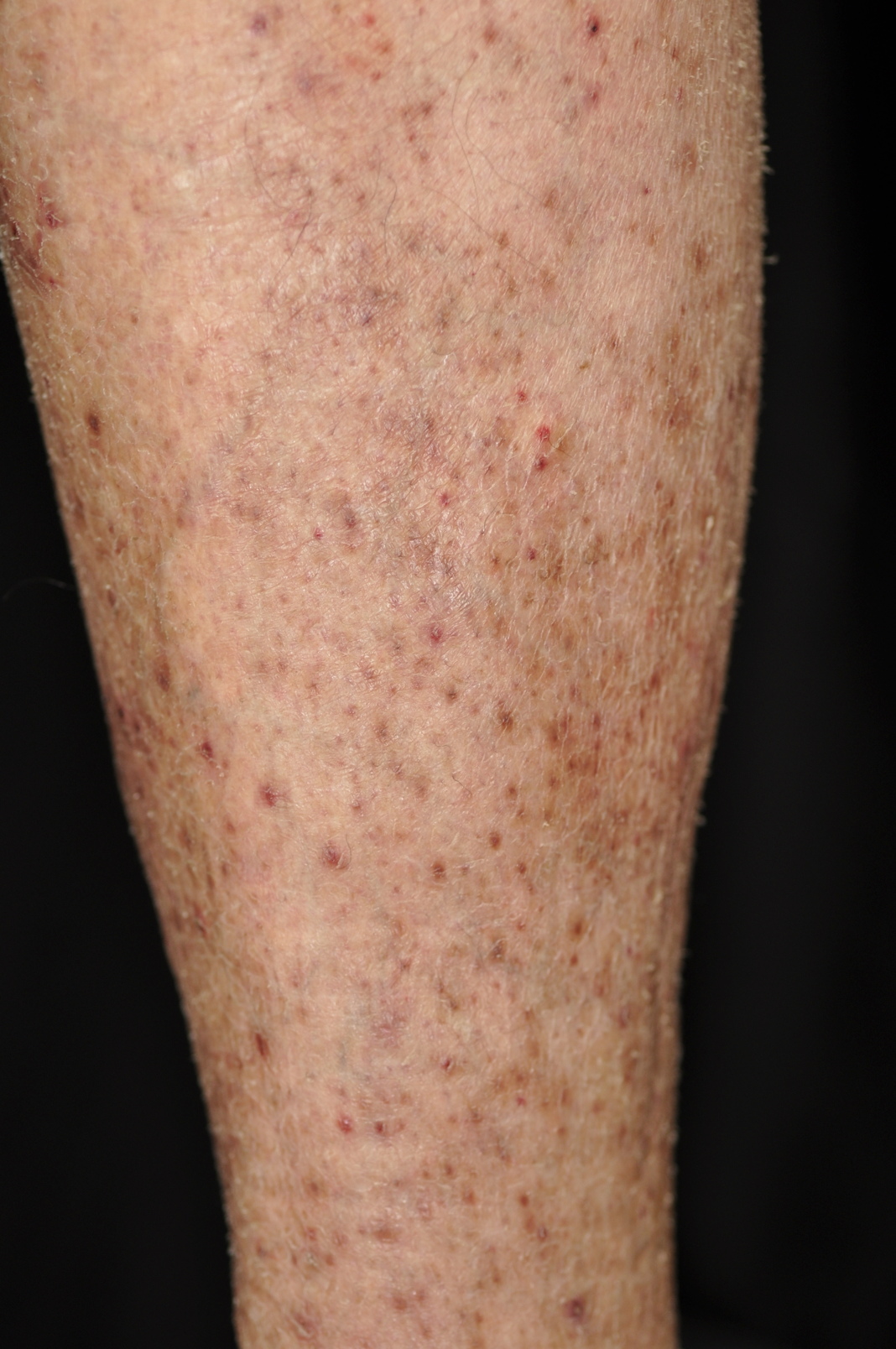
| Figure 1a. Alopecia with erythema and multiple pustules on the scalp. Figure 1b. Non-palpable purpura is notable on the lower leg. | |
A 79-year-old Japanese man suffering from adenocarcinoma of the lung was treated with erlotinib (Tarceva®) (150 mg daily). One month later, acneiform eruptions, paronychia, and alopecia appeared. Although he had some degree of male-pattern baldness before therapy, he complained of obvious and prominent hair loss along with the appearance of a number of pustules on the scalp after initiation of erlotinib. Physical examination revealed diffuse alopecia with multiple pustules on the top of his scalp (Figure 1a). The alopecia was clearly separated and accompanied by erythema, scales, and pustules. The pustules were also scattered on his cheeks and trunk. The bacterial and fungal cultures from the pustules were negative. He also presented with multiple purpuric macules on his lower legs and trunk (Figure 1b). He denied itching. Furthermore, paronychia of the right thumb and the left forefinger were observed. All of the eruptions appeared within 1 month after initiation of therapy with erlotinib.
 |
| Figure 2 |
|---|
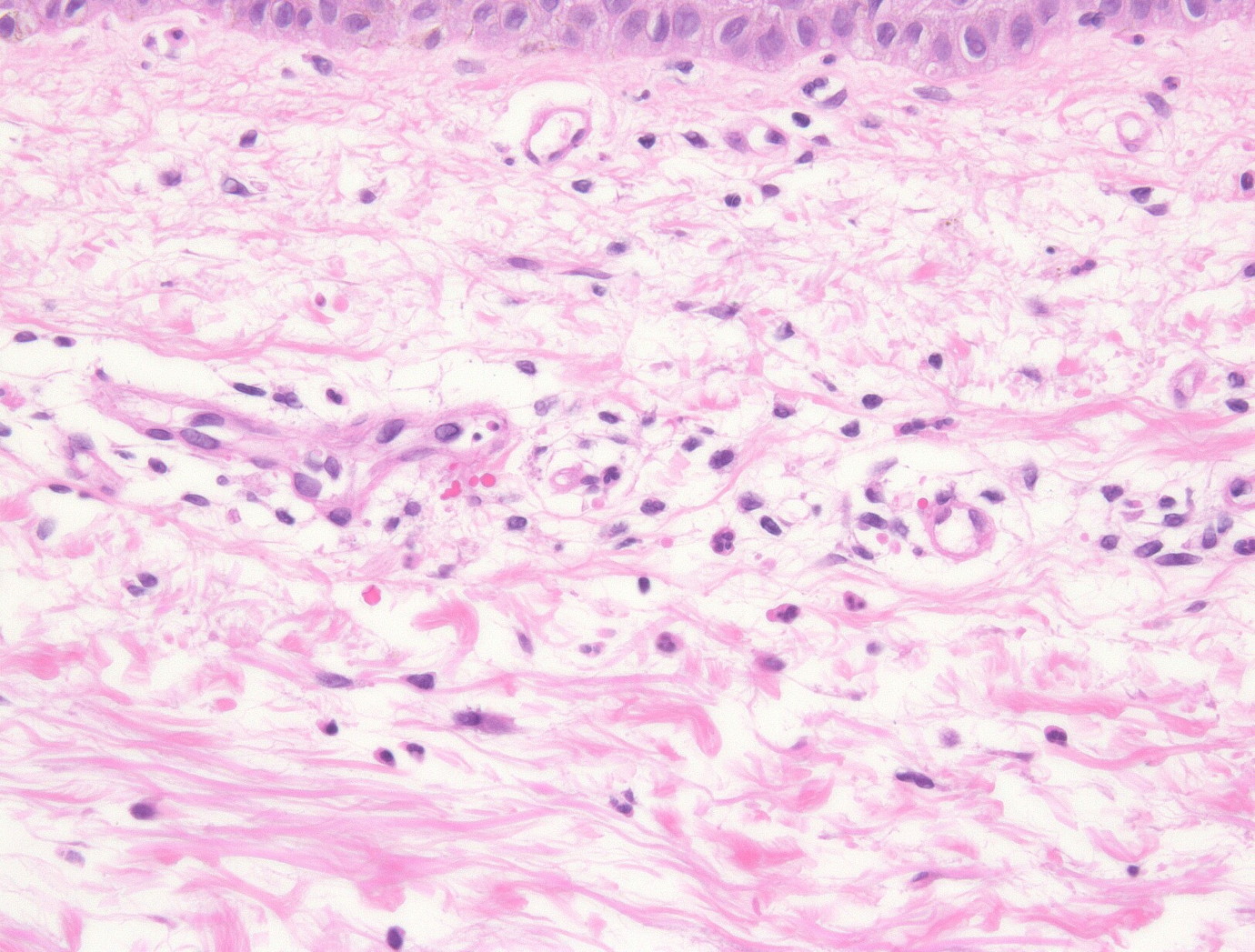
| Figure 2. Histopathological findings of a purpuric macule show extravasation of erythrocytes in the upper dermis. |
The histopathological findings of a purpuric macule taken from the leg revealed mild extravasation of erythrocytes in the upper dermis (Figure 2). Results of laboratory examination showed normal platelet counts. Liver and renal functions were normal. He was treated with oral minocycline (100 mg daily) and topical 1 percent clindamycin gel. The purpuric lesions on the lower legs have improved with pigmentation in spite of continuance of erlotinib, whereas pustular lesions with alopecia on the scalp are persistent.
Discussion
Adverse skin reactions are seen in 75 percent of patients treated with erlotinib, most of which develop within 3 weeks [1]. The most frequent skin reaction is an acneiform eruption, but xerosis, paronychia, hair changes, telangiectasia, and hyperpigmentation are also well-known [2]. On the contrary, purpuric drug eruption related to the EGF-R inhibitors is a rare skin reaction. So far, several reports that showed purpuric eruptions after treatment with gefitinib have been published; these included leukocytoclastic vasculitis [3, 4, 5, 6]. However, to our knowledge, a purpuric eruption associated with erlotinib has not been reported. Our case presented with purpuric lesions on the trunk as well as the lower legs. The purpuric lesions on the trunk were intermingled with folliculitis. The purpura was non-pruritic; itching and scratching were denied. Also, platelet counts were normal. Histologically, features of leukocytoclastic vasculitis were not observed.
In the skin, EGF-R is expressed by basal keratinocytes, sebocytes, the outer root sheath, and some endothelial cells; it plays a role in the normal differentiation and development of skin hair follicles and keratinocytes [7]. Inhibition to EGF-R on the endothelial cells of cutaneous vessels may contribute to induce minor vascular impairment and extravasation of erythrocytes, leading to a purpuric eruption [4]. On the other hand, EGF-R targeted therapy affects the immune response with increased inflammatory cell chemoattractants that results in recruitment of leukocytes, enzyme release, apoptosis, and tissue damage. Perivascular infiltrations lead to vessel wall damage that results in ectatic vessels and extravasation of erythrocytes [8]. Blume et al. [5] described the possibility that gefitinib produces an occlusive vasculopathy of the subcutaneous vascular system. This hypothesis is supported by the data showing increased platelet aggregation and thromboxane levels in patients treated with gefitinib [9]. Long after the condition of dermal congestion and platelet aggregation, extravasation may be induced and purpuric reactions can occur.
Another interesting feature in our case is diffuse alopecia with pustules on the scalp, which simultaneously occurred after starting erlotinib therapy. Alopecia has been reported in 5 percent of patients treated with EGF-R inhibitors [8]. Interestingly, EGF-R null mice exhibit alopecia [11] and skin grafts from EGF-R null mice onto nude mice that express EGF-R show follicles with an abundant inflammation; alopecia occurs by 10 weeks [12]. In patients with alopecia who have been treated with EGF-R inhibitors, the histological examination of the scalp shows a marked inflammatory infiltrate that consists of lymphocytes, plasma cells, and some neutrophils and eosinophils [13]. Scarring alopecia showing an increased number of telogen and catagen hairs with perifollicular chronic inflammation and perifollicular fibrosis is also reported [14]. Unfortunately, scalp histological examination was not carried out in our case because he refused skin biopsy from the scalp. In vitro models have shown that the activation of the EGF-R is involved in triggering the transition from anagen to catagen [15]. EGF-R has appeared to be an important mediator in order to enter into the catagen stage for the regulation of the hair cycle. Inhibition of EGF-R may result in the abnormalities of the hair cycle and increased production of inflammatory mediators.
In conclusion, alopecia with pustules and purpura were possibly induced by erlotinib therapy in our patient. We believe that further investigation is indispensable to understand the pathology of this phenomenon and that will contribute to the management of patients using EGF-R tyrosine kinase inhibitors.
References
1. Johnson JR, Cohen M, Sridhara R, Chen YF, Williams GM, Duan J, Gobburu J, Booth B, Benson K, Leighton J, Hsieh LS, Chidambaram N, Zimmerman P, Pazdur R. Approval summary for erlotinib for treatment of patients with locally advanced or metastatic non-small cell lung cancer after failure of at least one prior chemotherapy regimen. Clin Cancer Res. 11; 6414-6421, 2005. [PubMed]2. Segaert S, van Cutsem E. Clinical signs, pathophysiology and management of skin toxicity during therapy with epidermal growth factor receptor inhibitors. Ann Oncol. 16; 1425-33, 2005. [PubMed]
3. Kurokawa I, Endo K, Hirabayashi M. Purpuric drug eruption possibly due to gefitinib (Iressa®). Int J Dermatol. 44; 167-168, 2005. [PubMed]
4. Fernandez-Guarino M, Ryan AM, Perez-Garcia B, Gonzalez-Lopez C, Olasolo PJ. Necrotizing vasculitis due to gefitinib (Iressa®). Int J Dermatol. 46; 890-891, 2007. [PubMed]
5. Blume JE, Miller CC. Livedo reticularis with retiform purpura associated with gefitinib (Iressa®). Int J Dermatol. 46; 1307-1308, 2007. [PubMed]
6. Sheen YS, Hsiao CH, Chu CY. Severe purpuric xerotic dermatitis associated with gefitinib therapy. Arch Dermatol. 144; 269-270, 2008. [PubMed]
7. Van Doorn R, Kirtschig G, Scheffer E, Stoof TJ, Giaccone G. Follicular and epidermal alterations in patients treated with ZD1839 (Iressa), an inhibitor of the epidermal growth factor receptor. Br J Dermatol. 147; 598-601, 2002. [PubMed]
8. Lacouture ME. Mechanism of cutaneous toxicities to EGFR inhibitors. Nat Rev Cancer. 6; 803-812, 2006. [PubMed]
9. Kanazawa S, Yamaguchi K, Kinoshita Y, Muramatsu M, Komiyama Y, Nomura S. Gefitinib affects functions of platelet and blood vessels via changes in prostanoids balance. Clin Appl Thromb Hemost. 11; 429-434, 2005. [PubMed]
10. Perrotte P, Matsumoto T, Inoue K, Kuniyasu H, Eve BY, Hicklin DJ, Radinsky R, Dinney CP. Anti-epidermal growth factor receptor antibody C225 inhibits angiogenesis in human transitional cell carcinoma growing orthotopically in nude mice. Clin Cancer Res. 5; 257-265, 1999. [PubMed]
11. Murillass R, Larcher F, Conti CJ, Santos M, Ullrich A, Jorcano JL. Expression of dominant negative mutant of epidermal growth factor receptor in the epidermis of transgenic mice elicits striking alterations in hair follicle development and skin structure. EMBO J. 14; 5216-5223, 1995. [PubMed]
12. Hansen LA, Alexander N, Hogan ME, Sundberg LE, Dlugosz A, Threadgill DW, Magnuson T, Yuspa SH. Genetically null mice reveal a central role for epidermal growth factor receptor in the differentiation of the hair follicle and normal hair development. Am J Pathol. 150; 1959-1975, 1997. [PubMed]
13. Acharya J, Lyon C, Bottomley DM. Folliculitis-perifolliculitis related to erlotinib therapy spares previously irradiated skin. J Am Acad Dermatol. 60; 154-157, 2009. [PubMed]
14. Hepper DM, Wu P, Anadkat MJ. Scarring alopecia associated with the epidermal growth factor receptor inhibitor erlotinib. J Am Acad Dermatol. 64; 996-998, 2011. [PubMed]
15. Philpott MP, Kealey T. Effect of EGF on the morphology and patterns of DNA synthesis in isolated human hair follicules. J Invest Dermatol. 102; 186-191, 1994. [PubMed]
© 2012 Dermatology Online Journal