Granuloma faciale: Case report and review
Published Web Location
https://doi.org/10.5070/D355848902Main Content
Granuloma faciale: Case report and review
Jayantha Thiyanaratnam MD1, Sean D Doherty MD1, Bhuvaneswari Krishnan MD2,3, Sylvia Hsu MD1
Dermatology Online Journal 15 (12): 3
1. Department of Dermatology, Baylor College of Medicine, Houston, Texas shsu@bcm.edu2. Department of Pathology, Baylor College of Medicine, Houston, Texas
3. Michael E Debakey Veterans Affairs Medical Center, Houston, Texas
Abstract
Granuloma faciale (GF) is a rare benign chronic inflammatory dermatosis usually appearing only on the face. The lesions of GF typically present as single, asymptomatic, erythematous, non-changing nodules or plaques. We present an illustrative case of GF and briefly review available treatment options.
Case report
 |
| Figure 1 |
|---|
| Figure 1. 1.2 x 1.7 cm erythematous indurated plaque on the right nasal tip |
A 58-year-old Caucasian man with a history of rheumatoid arthritis and severe Raynaud phenomenon leading to fingertip necrosis and autoamputation of three fingertips in the past five years presented with an erythematous plaque on his nasal tip for the last 3 months. The plaque was asymptomatic, and the patient did not report a history of similar lesions or any other lesions on the body. Physical examination revealed a 1.2 x 1.7 cm erythematous indurated plaque on the right nasal tip (Fig 1).
 |  |
| Figure 2 | Figure 3 |
|---|---|
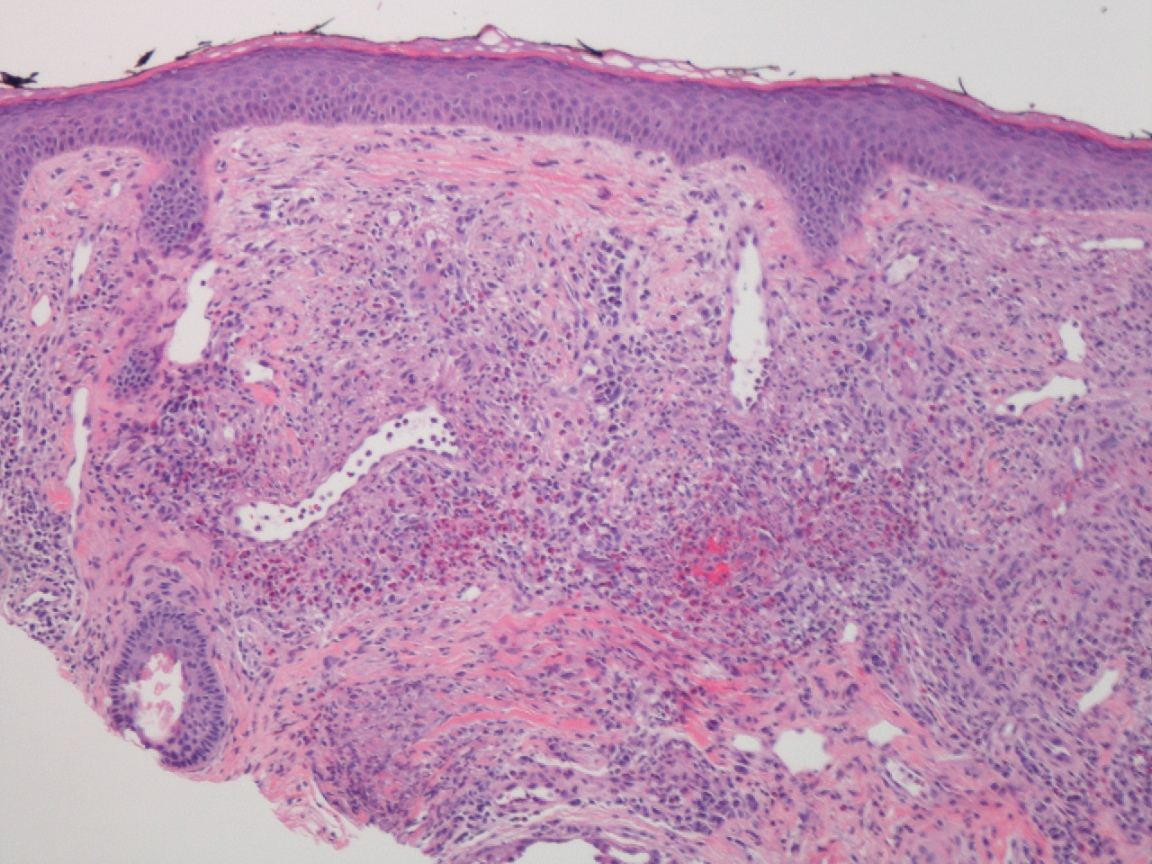
| Figure 2. Low power (x100) examination of the specimen revealed a dermal infiltrate and telangiectatic vessels with a grenz
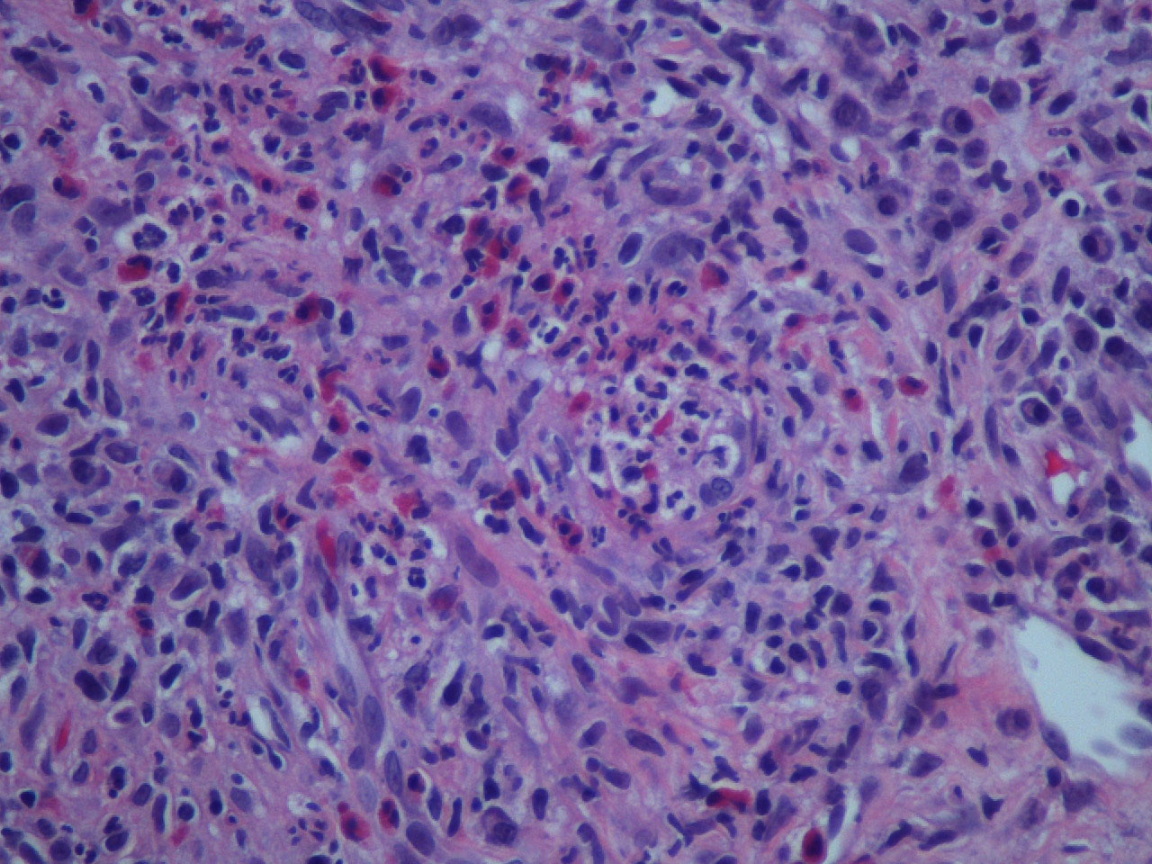
zone between the dermal infiltrate and a normal epidermis and adnexae. Figure 3. Examination of the dermal infiltrate under higher magnification revealed a polymorphous infiltrate consisting primarily of neutrophils, eosinophils, and plasma cells. Ectatic vessels were seen in the dermis with prominent endothelial cells and neutrophils in the vessel walls. | |
A biopsy of the lesion was performed and sent for histologic evaluation. Low power examination of the specimen (Fig. 2) revealed a dermal infiltrate and telangiectatic vessels with a grenz zone between the dermal infiltrate and a normal epidermis and adnexae. Examination of the dermal infiltrate under higher magnification (Fig. 3) revealed a polymorphous infiltrate consisting primarily of neutrophils, eosinophils, and plasma cells. Ectatic vessels were seen in the dermis with prominent endothelial cells and neutrophils in the vessel walls.
Based on these histologic findings, a diagnosis of GF was made. The patient returned for follow-up and was treated with 0.5 cc of intralesional triamcinolone 4 mg/cc. He was also started on tacrolimus ointment 0.1 percent twice daily. Three months after starting therapy, the patient had moderate improvement in clinical appearance of the lesion and opted to continue using the tacrolimus topically because he was very happy with the aesthetic improvement.
Discussion
Granuloma faciale most often occurs in middle-aged Caucasian men [1]. Clinically, the lesions appear as well-circumscribed smooth erythematous papules, nodules, or plaques that may increase in size and number. Once fully developed, GF usually does not change [2]. Granuloma faciale has an unknown etiology, but possible predisposing factors include actinic exposure, radiation [3], trauma, allergy [2], or an Arthus-like reaction [1]. Ninety-two percent of patients with GF have facial lesions only [4]. The most common locations are the cheeks, the forehead, the helix, the preauricular area, and the tips and sides of the nose. Extrafacial lesions, if present, usually appear months to years after the onset of facial lesions [1].
Confirmatory diagnosis of GF is made by histologic evaluation of the lesion. The epidermis is unaffected and is separated from the affected dermis by a grenz zone of normal dermal collagen. There is a polymorphous dense dermal infiltrate below the grenz zone consisting of neutrophils, lymphocytes, eosinophils, and plasma cells [5].
Granuloma faciale is a misnomer because its histologic appearance does not demonstrate granulomatous inflammation. Not all lesions reveal a grenz zone, and Ortonne et al. [6] reported in a series of 66 patients that 26 percent of lesions did not demonstrate this characteristic finding. Several reports have shown the presence of immune complexes in the walls of dermal blood vessels and the basement membrane zone [1], and vasculitis is variably reported in these lesions with Ortonne et al. [6] reporting vasculitis in 69 percent of lesions studied. Blood counts, chest radiographs, liver and kidney function tests are usually within normal limits [4].
Although the pathophysiology of GF is unknown, it has been suggested that it is mediated by interferon (IFN)-γ produced by CD4+ T-helper cells. Tacrolimus is a topical calcineurin inhibitor that decreases the upregulation of interleukin-2 and decreases T-cell activation. This reduction in T-cell activation leads to decreased production of IFN-γ and may explain the potential utility of topical tacrolimus in treating GF [7].
Tomson et al. [7] described two patients treated with topical tacrolimus: patient 1 used topical tacrolimus 0.1 percent twice daily and had resolution by 6 months. Treatment was then stopped, and the lesion returned one year later, so tacrolimus was re-started. Patient 2 showed resolution with topical tacrolimus 0.03 percent twice daily by 6 months with no recurrence three years later [7].
There is no standard therapy for GF because no treatments are reliably efficacious. Numerous therapies have been tried for GF including dapsone, oral immunosuppressants [2], pulse dye lasers [5], and surgical excision [8]. Our patient demonstrated a moderate response to topical tacrolimus therapy and may continue to demonstrate improvement when treatment is continued for a longer duration.
References
1. Rossiello L, Palla M, Aiello FS, Baroni A, Satriano RA. Granuloma faciale with extrafacial lesions. Skinmed 2007;6:150-151. [PubMed]2. Nigar E, Dhillon R, Carr E, Matin RN. Eosinophilic angiocentric fibrosis and extrafacial granuloma faciale. Histopathology 2007;51:729-731. [PubMed]
3. Chung WK, Park GH, Kim CH, Chang SE, Lee MW, Choi JH, Moon KC, Koh JK. Keloidal granuloma faciale after CO2 laser treatment for melanocytic naevus. J Eur Acad Dermatol Venereol 2009;23:611-612. [PubMed]
4. De D, Kanwar AJ, Radotra BD, Gupta S. Extrafacial granuloma faciale: report of a case. J Eur Acad Dermatol Venereol 2007;21:1284-1286. [PubMed]
5. LeBoit PE. Granuloma faciale: a diagnosis deserving of dignity. Am J Dermatopathol 2002;24:440-443. [PubMed]
6. Ortonne N, Wechsler J, Bagot M, Grosshans E, Cribier B. Granuloma faciale: a clinicopathologic study of 66 patients. J Am Acad Dermatol 2005;53:1002-9. [PubMed]
7. Tomson N, Sterling JC, Salvary I. Granuloma faciale treated successfully with topical tacrolimus. Clin Exp Dermatol 2009;34:424-425. [PubMed]
8. Requena C, Castejón P, Sanmartín O, Botella-Estrada R, Nagore E, Serra-Guillén C, Sorní G, Guillén C. Rhinophyma-like granuloma faciale. J Eur Acad Dermatol Venereol 2006;20:881-882. [PubMed]
© 2009 Dermatology Online Journal