Linear porokeratosis
Published Web Location
https://doi.org/10.5070/D34t28r2kwMain Content
Linear porokeratosis
Carolyn Kim MD
Dermatology Online Journal 11 (4): 22
Department of Dermatology, New York University School of Medicine
Abstract
A 66-year-old man presented with linear lesions of 5-years duration on his right lower extremity along Blaschko's lines. Physical examination showed hyperpigmented and violaceous papules with hypopigmented centers that were surrounded by fine, raised hyperkeratototic rims. The lesions were characteristic of porokeratosis, and the diagnosis was confirmed by histopathological examination. Associated medical conditions and treatment modalities are reviewed.
A 66-year-old Peruvian man presented to the Dermatology Clinic at Bellevue Hospital Center for evaluation and treatment of a pruritic lesions present for five years on his right leg. Previous treatment included urea cream, steroid cream, and tretinoin cream. There was no improvement with use of any of the topical preparations.
Numerous, hyperpigmented, violaceous, round papules, some coalescing into plaques, extended from the perianal region onto the leg along Blaschko's lines. Many of the papules and plaques had an annular appearance, with thin, raised, hyperkeratotic borders that surrounded central hypopigmented and depressed areas.

|
|
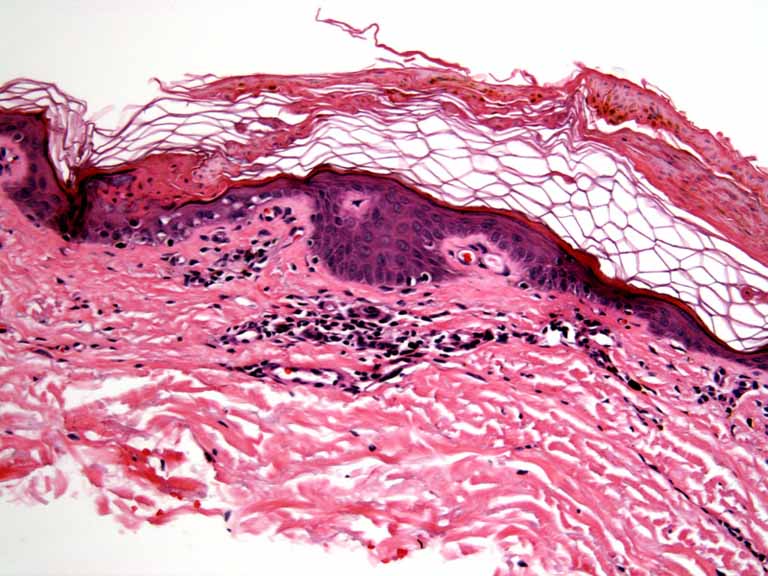
| Figure 1 | Figure 2 |
|---|
Histopathology reveals a thin tier of parakeratosis beneath which is a diminished granular-cell layer and a superficial band-like lymphocytic infiltrate.
Comment
The clinical variants of porokeratosis include porokeratosis of Mibelli, disseminated superficial actinic porokeratosis (DSAP), linear porokeratosis, punctate porokeratosis, and porokeratosis palmaris et plantaris disseminata. Some cases of porokeratosis are inherited in an autosomal dominant manner, and others have no family history. Linear porokeratosis, which is often congenital, is the mosaic form of the autosomal dominant condition [1].
The diagnosis of classic porokeratosis is usually apparent; the thread-like elevated rim encompasses the central area and creates an annular configuration. The cornoid lamella on histopathologic examination corresponds clinically to the distinct, peripheral, raised, hyperkeratotic ridge. The histopathologic patterns are similar in all forms of porokeratosis. Overexpression of p53 tumor-suppressor protein has been found in porokeratosis [2].
The development of Bowen's disease and squamous-cell carcinoma within the lesions of porokeratosis is well documented, with rare occurrences of metastasis and death [3, 4]. Squamous-cell carcinomas arising from porokeratosis in organ-transplant recipients also are described [5, 6]. Other medical conditions that have been reported in association with porokeratosis include immunosuppression, being a recipient of organ transplantation, burn scars, Crohn's disease, and end-stage liver disease [7, 8, 9, 10].
Available treatment options include topical medications such as 5-fluorouracil, imiquimod, and retinoids, as well as the destructive modalities such as cryotherapy, CO2 laser, curettage, excision, and dermabrasion. Oral acitretin has been used to decrease the extent of the disease, but the lesions recur upon its discontinuation [11].
References
1. Pearson D, et al. Benign epidermal tumors and proliferations. In Bolognia JL, et al., eds. Dermatology. Edinburgh: Mosby, 2003:17072. Johnson B, Honig P. Congenital diseases (genodermatoses). In: Elder D, et al., eds. Lever's Histopathology of the Skin. 8th edition. Philadelphia: Lippincott, Williams and Wilkins, 1997:117
3. Rongioletti F, Rebora A. Disseminated porokeratosis with fatal metastatic squamous cell carcinoma: and additional case of "malignant disseminated porokeratosis". Am J Dermatopathol 2002; 24:144
4. Lozinski AZ, et al. Metastatic squamous cell carcinoma in linear porokeratosis of Mibelli. J Am Acad Dermatol 2003; 16:448.
5. Silver SG, et al. Fatal squamous cell carcinoma arising from transplant-associated porokeratosis. J Am Acad Dermatol 2003; 49:931
6. Anzai S, et al. Squamous cell carcinoma in a renal transplant recipient with linear porokeratosis. J Dermatol 1999; 26:244
7. Kanitakis J, et al. Porokeratosis in organ transplant recipients. J Am Acad Dermatol 2001; 44:144
8. Nova MP, et al. Porokeratosis arising in a burn scar. J Am Acad Dermatol 1991; 25:354
9. Morton CA, et al. Porokeratosis and Crohn's disease. J Am Acad Dermatol 1995; 32:894
10. Hunt SJ, et al. Linear and punctate porokeratosis associated with end-stage liver disease. J Am Acad Dermatol 1991; 25:937
11. Goldman, GD, Milstone LM. Generalized linear porokeratosis treated with etretinate. Arch Dermatol 1995; 131:496
© 2005 Dermatology Online Journal