Annular erythematous papules in the neckline
Published Web Location
https://doi.org/10.5070/D34ps3r109Main Content
Annular erythematous papules in the neckline
MJ Espiñeira-Carmona, S Arias-Santiago, J Aneiros-Fernández, MA Fernández-Pugnaire, R Naranjo-Sintes, J Aneiros-Cachaza
Dermatology Online Journal 17 (1): 7
Dermatology and Pathology Department, San Cecilio University Hospital, Granada, Spain. Mariapepa84@hotmail.comAbstract
A 45-year-old woman with personal history of hypertension presented with an erythematous lesion in the neckline for a year and with a progressive growth. A physical examination revealed an annular lesion with erythematous papules in the edge. Histological exam showed phagocytosis of elastic fibers by multinucleated cells compatible with annular elastolytic giant-cell granuloma. The patient did not present any other associated systemic manifestation. Treatment with tacrolimus 0.1 percent ointment was prescribed with a very good response after two months.
Case synopsis
 |
| Figure 1 |
|---|
| Figure 1. Papules and plaques with annular distribution and central atrophy and raised erythematous margins in the neckline |
A 45-year-old woman with personal history of hypertension presented with a slightly pruritic and erythematous lesion in the neckline for a year with a progressive growth. Her family history was negative for skin problems. A physical examination revealed papules and plaques with annular distribution and central atrophy and raised erythematous margins in the neckline (Figure 1). The patient did not present any other associated systemic manifestation and there was no mucous membrane or nail involvement. Histologic sections are shown in figures 2 and 3.
 |  |
| Figure 2 | Figure 3 |
|---|---|
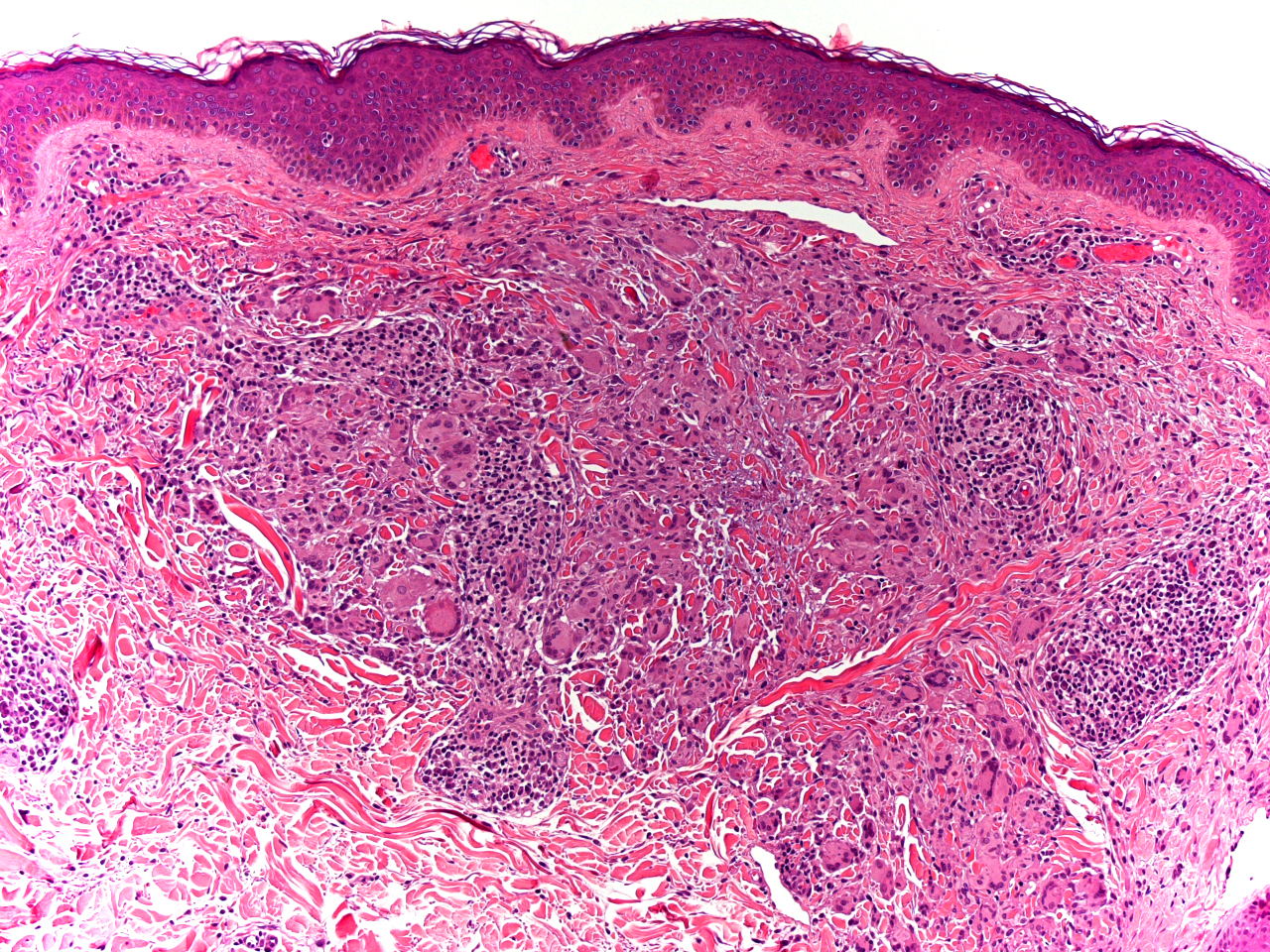
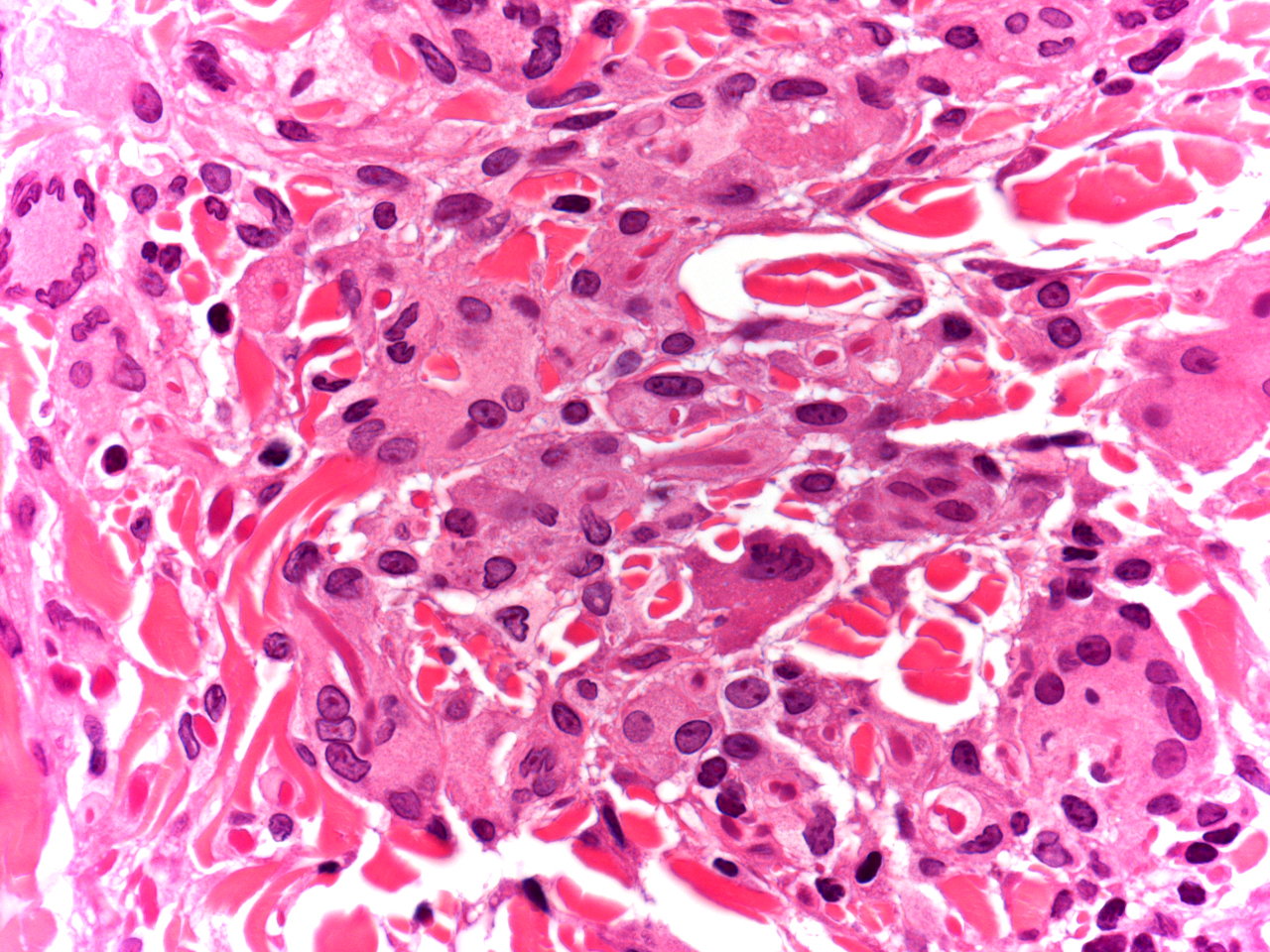
| Figures 2 & 3. Granulomatous infiltrate without palisading composed mainly of multinucleated giant cells located in upper reticular dermis | |
Microscopic findings and clinical course
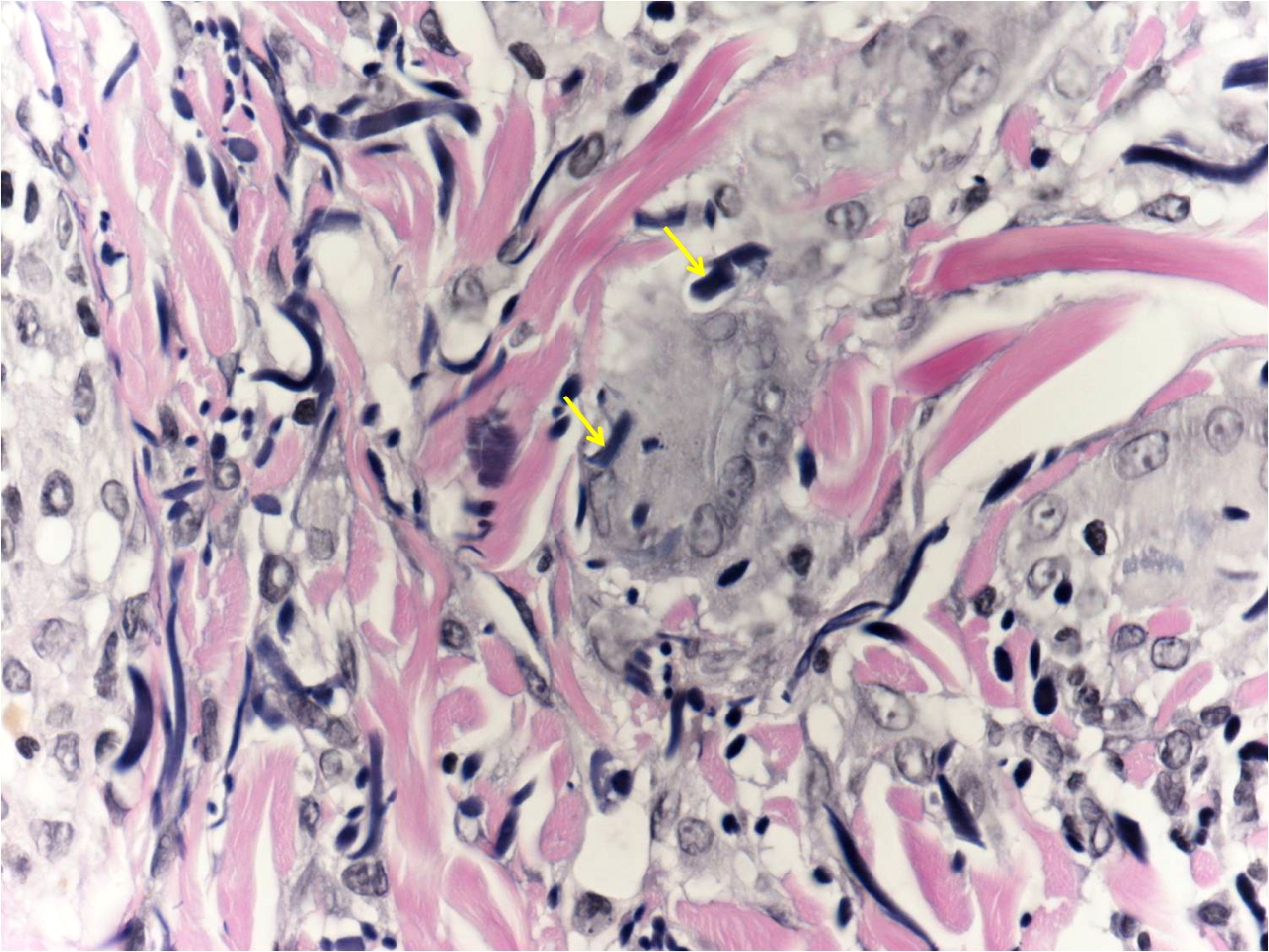
Histological study revealed a granulomatous infiltrate without palisading composed mainly of multinucleated giant cells located in upper reticular dermis. Necrobiosis or excessive deposit of mucosubstances were not appreciated (Figures 2 and 3). With orcein staining fragmentation of elastic fibers, elastopahogocytosis, and loss of elastic fibers in the center of the lesion were noticed (Figure 4). Treatment with tacrolimus 0.1 percent ointment was prescribed with a very good response after two months (Figure 5).
 |  |
| Figure 4 | Figure 5 |
|---|---|
| Figure 4. Elastopahogocytosis and loss of elastic fibers in the center of the lesion (orcein staining) Figure 5. Treatment with tacrolimus 0.1 percent ointment was prescribed with a very good response after two months | |
Discussion
There are several etiologically unrelated diseases that present with annular morphology, which may require histological evaluation for the differential diagnosis. Sometimes lesions clinically similar to granuloma annulare (GA) show atypical histological features like a significant degree of elastolysis and elastofagocitosis by multinucleated giant cells without necrobiosis or excessive deposit of mucosubstances [1]. O'Brien in 1975 described these findings in sun-exposed areas of the skin and suggested the term actinic granuloma, explaining the role of sunlight in the etiology of this lesion, which could lead to alterations in elastic fibers causing a granulomatous reaction [2]. In 1979 Hanke described lesions that were very similar clinically and histologically, but with no solar elastosis and located in non-photo exposed areas. He argued that solar elastosis was not always present [3] and proposed the more descriptive term of annular elastolytic giant-cell granuloma (AEGCG), which is widely used today and replaced the previously ones as O'Brien actinic granuloma, atypical necrobiosis lipoidica or disciform Miescher granuloma [3].
The AEGCG is characterized histologically by a non palisading granulomatous infiltrate with multinucleated giant cells in the upper dermis. Fragmentation of elastic fibers, elastopahogocytosis, and loss of elastic fibers are common findings. Necrosis, necrobiosis or an increase of mucosubstances are not appreciate [1]. These features help to distinguish AEGCG from granuloma annulare and necrobiosis lipoidica, which are the main disorders in the histological differential diagnosis.
Clinical features described by Hanke are papular lesions isolated or grouped in rings mainly in photoexposed areas [3], they occur more frequently in females and the mean age of onset is between 30 and 50 years [4]. Also cases in children and in people over 70 years have been reported [5, 6, 7, 8, 9], and their location in non-photoexposed areas [7, 10].
Although the etiology and pathogenesis of AEGCG are not fully understood it is believed that solar radiation, heat, or other factors lead to the alteration of elastic fibers precipitating an immune response and granuloma formation [8]. Several authors suggest that AEGCG and mid-dermal elastolysis may represent different stages of the clinical spectrum of dermal elastolysis. After an elastofagocytosis inflammatory phase by multinucleated giant cell is followed by a phase of loss of elastic fibers in the reticular dermis [12, 13].
There have been reported cases of AEGCG associated with diabetes, sarcoidosis, and hematological malignancies [4, 11]. This disease presents a chronic evolution, however spontaneous remission has been documented [14]. Treatment is empirical, variable results have been reported with therapies such as: oral steroids [2], antimalarial [15], PUVA [4], cyclosporine [16], tranilast alone [9] or combined with pimecrolimus [6], and topical tacrolimus [11].
In our patient treatment with tacrolimus 0.1 percent ointment was prescribed with a very good response after two months. Previous studies show a good response to calcineurin inhibitors [6, 11].
A clinical case of AEGCG has been presented with a very good response to topical tacrolimus avoiding the adverse effects of other systemic therapies.
References
1. Limas C. The spectrum of primary cutaneous elastolytic granulomas and their distinction from granuloma annulare: a clinicopathological analysis. Histopathology 2004 Mar; 44(3):277-82 [PubMed]2. O'Brien JP. Actinic granuloma: an annular connective tissue disorder affecting sun- and heat-damaged (elastotic) tissue. Arch. Dermatol 1975; 111; 460-466. [PubMed]
3. Hanke CW, Bailin PL, Roenigk HH. Annular elastolytic giant cell granuloma. A clinicopathologic study of five cases and a review of similar entities. J Am Acad Dermatol. 1979 Nov;1(5):413-21 [PubMed]
4. Djilali-Bouzina F, Grange F, Krzisch S, Schnebelen MP, Grosshans E, Guillaume JC. Annular elastolytic giant cell granuloma. Ann Dermatol Venereol. 2010 Aug-Sep;137(8-9):536-40. [PubMed]
5. Herron MD, Coffin CM, Vanderhooft SL. Annular elastolytic cell granuloma, Pediatr Dev Pathol 2002.5:305-9.
6. Lee HW, Lee MW, Choi JH, Moon KC, Koh JK. Annular elastolytic giant cell granuloma in an infant: Improvement after treatment with oral tranilast and topical pimecrolimus. J Am Acad Dermatol. 2005 Nov;53(5 Suppl 1):S244-6. [PubMed]
7. Ishibashi A, Yokoyama A, Hirano K. Annular elastolytic giant cell granuloma occurring in covered areas, Dermatologica. 1987; 174(6): 293-7 [PubMed]
8. Ventura F, Vilarihno C, da Luz Duarte M, Pardal F, Brito C. Two cases of annular elastolytic giant cell granuloma: Different response to the treatment. Dermatol Online J. 2010 Mar 15;16(3):11. [PubMed]
9. Morita K, Okamoto H, Miyachi Y. Papular elastolytic giant cell granuloma: a clinical variant of annular elastolytic giant cell granuloma or generalized granuloma annulare? Eur J Dermatol 1999; 9: 647-9. [PubMed]
10. Campos-Muñoz L, Díaz-Díaz RM, Quesada-Cortés A, Hernández-Cano N, Martín-Díaz MA, Regojo-Zapata RM, Casado Jiménez M. Annular elastolytic giant cell granuloma: a case report located in non-sun exposed areas. Actas Dermosifiliogr. 2006 Oct;97(8):533-5. [PubMed]
11. Rongioletti F, Baldari M, Burlando M, Parodi A. Papular elastolytic giant cell granuloma: report of a case associated with monoclonal gammopathy and responsive to topical tacrolimus. Clin Exp Dermatol. 2010 Mar;35(2):145-8 [PubMed]
12. Müller FB, Groth W. Annular elastolytic giant cell granuloma: a prodromal stage of mid-dermal elastolysis? Br J Dermatol. 2007 Jun;156(6):1377-9. [PubMed]
13. Hohenleutner S, Wlotzke U, Landthaler M, Stolz W. Elastolysis of the mid-dermis and annular elastolytic giant cell granuloma: different stages in the clinical spectrum of dermal elastolysis? Case report and review of the literature. Hautarzt. 1997 Jan;48(1):45-50. [PubMed]
14. Ragaz A, Ackerman AB. Is actinic granuloma a specifit condition? Another view: perhaps the concept should be extended. Am J Dermatopathol. 1979;1:51-3.
15. Hermes B, Haas N, Czarnetzki BM. Elastolytic giant cell granuloma annulare with spontaneous healing tendency. Hautarzt. 1995 Jul;46(7):490-3. [PubMed]
16. Ozkaya Bayazit E, Buyukbabani N, Baykal C, Ozturk A, Okucu M, Soyer H. Annular elastolytic giant cell granuloma: sparing of a burn scar and successful treatment with chloroquine. Br J Dermatol. 1999 Mar; 140(3): 525-30. [PubMed]
17. Tsutsui K, Hirone T, Kubo K, Matsui Y. Annular elastolytic giant cell granuloma: response to cyclosporin A. J Dermatol 1994 Jun;21(6):426-429. [PubMed]
© 2011 Dermatology Online Journal