Axillary syringomas
Published Web Location
https://doi.org/10.5070/D34jt089htMain Content
Axillary Syringomas
Neda Nosrati MD1, Neil M Coleman MD2, Sylvia Hsu MD1
Dermatology Online Journal 14 (4): 13
1. Department of Dermatology, Baylor College of Medicine, Houston, TX2. Department of Pathology, Baylor College of Medicine, Houston, TX. shsu@bcm.edu
Abstract
Syringomas are common benign neoplasms encountered mostly around the eyes. However, as described herein, these tumors can occur in atypical locations such as the axilla. The differential diagnosis revolves around those entities more likely seen in this anatomical location (such as Fox-Fordyce, Hailey-Hailey and Darier diseases). Various ablative modalities are curative.
Case Report
 |
| Figure 1 |
|---|
| Figure 1. Tan-colored papules in axilla |
A 24-year-old woman presented with a 10-year history of asymptomatic papules in her axillae. She was otherwise healthy and denied taking any medications. She denied a family history of similar lesions in the axillae or the eyelids. On examination, there were several tan-colored papules in the bilateral axillae (Fig. 1). There were no papules on her eyelids. A 4-mm punch biopsy was obtained. Histopathology showed epithelial strands and small ducts in the dermis, some with a "tadpole" configuration, consistent with syringoma (Figs. 2 and 3).
 | 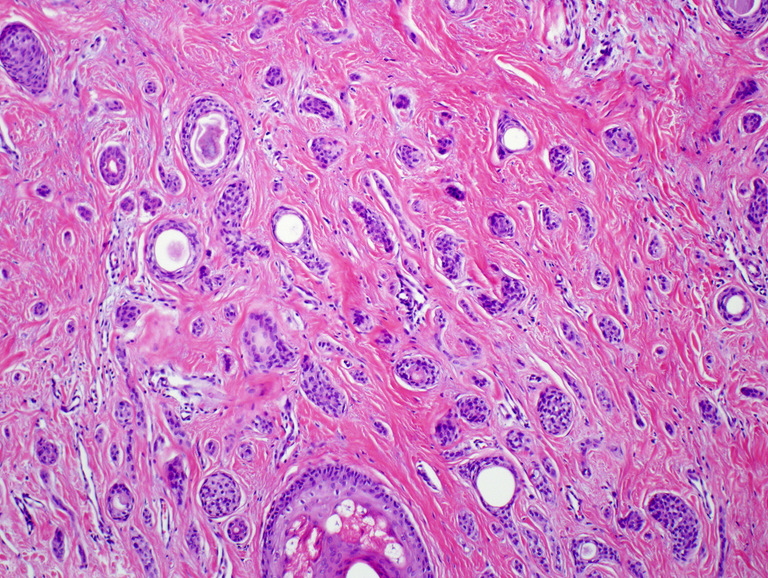 |
| Figure 2 | Figure 3 |
|---|---|
| Figure 2a. Epithelial strands and small ducts dispersed in a fibrous stroma (H&E 40X) Figure 2b. Some ducts have a "tadpole" appearance (H&E 100X) | |
Discussion
Syringomas are benign sweat gland tumors, which originate from the straight portion of the intradermal eccrine sweat duct. Eccrine sweat ducts are distributed widely in the skin; however, these tumors are usually found in the head and neck region, most often on the eyelids [1]. Less commonly they can be seen on the scalp, forehead, cheeks, axillae, abdomen, extremities, genitalia, and buttocks [2]. Clinically, they present as small, firm, skin-colored, yellow, or brown papules [2, 3]. Syringomas are encountered more frequently in women with a female to male ratio of approximately 2:1 according to most studies [4], although some quote a ratio as high as 6.6:1 [5]. Most often they occur during puberty or the third and fourth decades of life [2]. There is a more rare eruptive form in which the lesions present in large numbers and in successive crops on the anterior chest, neck, upper abdomen, axillae, and periumbilical region [2, 4].
On histology, syringomas have a symmetrical, well-circumscribed appearance and are confined to the upper dermis with no connection to the overlying epidermis [1]. Epithelial cell proliferations are arranged in cords, nests, or tubules, which can display the characteristic "comma" or "tadpole" shapes, and are all embedded in a fibrous stroma [1, 2]. Monomorphous cuboidal epithelial cells with small normochromic nuclei and a small to moderate amount of pale eosinophilic cytoplasm line the tubules in a single or double layer. There is a subset of tumors in which the neoplastic cells display abundant clear cytoplasm [1].
There is some debate over the eccrine origin of syringomas as most are located in apocrine rich areas such as the lower eyelid, axillae, and abdomen, rarely occurring in eccrine only areas like the palms and soles [6]. However, immunohistochemical studies have shown the presence of several enzymes including succinic dehydrogenase, aminophosphorylase, periodic acid-Schiff-positive material, and leucine aminopeptidase all of which are more highly concentrated within eccrine ducts as compared to apocrine [7]. Furthermore, syringomas exhibit a marker pattern that is very similar to that seen in normal dermal eccrine ducts with epithelial membrane antigen in peripheral cells, cytokeratin (CK) 10 in intermediate cells, and CK 6, CK 19, and carcinoembryonic antigen in luminal cells [8].
Current evidence supports the theory that syringomas may be under hormonal control. Immunohistochemical studies have detected progesterone and estrogen receptors within these tumors. The presence of these hormone receptors may explain why syringomas are more common in females and have a peak incidence during puberty [9]. Furthermore, there are reports that have shown an increase in tumor size during pregnancy and menstration [3]. However, a recent study from Korea of 61 patients with syringoma described only one patient experiencing an exacerbation of her symptoms during menstruation [5]. In their study they found that summer season or high temperature was the most common aggravating factor [5].
The differential diagnosis for axillary syringomas includes disorders that also present with skin-colored to brown papules in the axillae such as Darier disease, Fox-Fordyce disease, Hailey-Hailey disease, flat warts, and keratosis pilaris [10]. Darier disease affects several areas simultaneously such as the axillae, upper chest area, back, ears, nasolabial folds, forehead, scalp, and groin. The lesions of Darier disease can be greasy, scaly, crusted, and keratotic; also the disease has characteristic nail changes [10]. Hailey-Hailey disease has a varied morphology, but in general it is a blistering disease, which can present with episodic macerations and erosions in intertriginous areas. The lesions of Fox-Fordyce disease are small infundibulocentric papules that may have a central keratotic plug and yellow color [11].
Syringoma should be distinguished from its rare malignant counterparts such as microcystic adnexal carcinoma and syringoid eccrine carcinoma [1]. Syringoid eccrine carcinoma is a slow growing, but locally invasive tumor that can metastasize to regional lymph nodes and consequently to bone. Histologically, it is very similar to syringoma, but can be differentiated by its cellularity, anaplasia, and deep invasiveness [12]. Microcystic adnexal carcinoma is a locally aggressive neoplasm that can clinically be confused with benign adnexal tumors, especially syringomas. Goldstein et al. [13] reported six cases that initially displayed benign histology but were later found to invade deep into skeletal muscle and perineural spaces causing tissue destruction. Syringomas can be distinguished from microcystic adnexal carcinomas by infrequent calcification, lack of prominent horn cyst formation, and infrequent single file strand formation. Furthermore, syringomas, unlike microcystic adnexal carcinoma, do not exhibit subcutaneous or perineural involvement [13].
Syringomas are benign, mostly asymptomatic and are treated mainly for cosmetic purposes. There are multiple treatment options currently available, which include surgical methods such as excision, cryosurgery, dermabrasion, electrodesiccation with and without curettage, carbon dioxide laser, and chemical peels [14, 15]. Unfortunately, many of these treatments can lead to scarring or pigmentary changes especially because these tumors lie deep in the dermis. A new study by Park et al. [14] proposes the use of a multiple-drilling method using the carbon dioxide laser to make several small holes in each lesion. They found this technique to be safe, easy, and effective in the 11 patients who were treated in their study. Furthermore, they had no incidence of scarring or pigmentary changes after 1-29 months of follow-up [14].
This case is of interest as our patient has an unusual distribution. To our knowledge, there is only one previous case cited in the literature [10].
References
1. Obaidat NA, Alsaad KO, Ghazarian D. Skin adnexal neoplasms-part 2: An approach to tumours of cutaneous sweat glands. J Clin Pathol 2007;60:145-159. PubMed2. Nguyen DB, Patterson JW, Wilson BB. Syringoma of the moustache area. J Am Acad Dermatol 2003;49:337-9. PubMed
3. Bal N, Aslan E, Kayaselcuk F, Tarim E, Tuncer I. Vulvar Syringoma Aggravated by Pregnancy. Pathol Oncol Res 2003;9(3):196-7. PubMed
4. Weiss E, Paez E, Greenberg AS, San Juan E, Fundaminsky M, Helfman TA. Eruptive syringomas associated with milia. Int J Dermatol 1995;34:193-5. PubMed
5. Lee JH, Chang JY, Lee KH. Syringoma: a clinicopathologic and immunohistologid study and results of treatment. Yonsei Med J 2007;48(1):35-40. PubMed
6. Paquette DL, Massa MC. An unusual presentation of syringomas on the buttocks. J Am Acad Dermatol 1998;39(6):1032-3. PubMed
7. Hashimoto K, Gross B, Lever WF. Syringoma: histochemical and electron microscopic studies. J Invest Dermatol 1966;46:150-166. PubMed
8. Demirkesen C, Hoede N, Moll R. Epithelial markers and differentiation in adnexal neoplasms of the skin: an immunohistochemical study including individual cytokeratins. J Cutan Pathol 1995;22(6):518-535. PubMed
9. Wallace ML, Smoller BR. Progesterone receptor positivity supports hormonal control of syringomas. J Cutan Pathol 1995;22(5):442-5. PubMed
10. Kakinuma H, Urahashi J. Multiple Axillary Papules-Quiz Case. Arch Dermatol 2004;140(9):1161-8. PubMed
11. Boer A. Patterns Histopathologic of Fox-Fordyce Disease. Am J Dermatopathol 2004;26(6):482-492. PubMed
12. Nishizawa A, Nakanishi Y, Sasajima Y, Yamazaki N, Yamamoto A. Syringoid eccrine carcinoma with apparently aggressive transformation: case report and review of the literature. Int J Dermatol 2006;45(10):1218-1221. PubMed
13. Goldstein DJ, Barr RJ, Santa Cruz DJ. Microcystic Adnexal Carcinoma: A Distinct Clinicopathologic Entity. Cancer 1982;50:566-572. PubMed
14. Park HJ, Lee DY, Lee JH, Yang JM, Lee ES, Kim WS. The Treatment of Syringomas by CO(2) Laser Using a Multiple-Drilling Method. Dermatol Surg 2007;33:310-313. PubMed
15. Aradi IK. Periobital Syringoma: A pilot study of the efficacy of low-voltage electrocoagulation. Dermatol Surg 2006;32:1244-1250. PubMed
© 2008 Dermatology Online Journal