Acne in Adolescents: Quality of Life, Self-Esteem, Mood and Psychological Disorders
Published Web Location
https://doi.org/10.5070/D34hp8n68pMain Content
Acne in Adolescents: Quality of life, self-esteem, mood, and psychological disorders
Lauren K Dunn PhD1, Jenna L O’Neill MD1, Steven R Feldman MD PhD1,2,3
Dermatology Online Journal 17 (1): 1
1. Department of Dermatology2. Department of Pathology
3. Department of Public Health Sciences
Center for Dermatology Research, Wake Forest University School of Medicine, Winston-Salem, North Carolina. sfeldman@wfubmc.edu
Abstract
INTRODUCTION: Acne is a significant adolescent problem and may precipitate emotional and psychological effects. The impact of acne on psychological parameters and implications for acne treatment are not fully understood. METHODS: We performed a MEDLINE search using the terms “acne” and “adolescent” along with “psychological,” “depression,” or “psychiatric,” which yielded 16 reviewed studies. RESULTS: Qualitative review of the selected articles revealed that the presence of acne has a significant impact on self-esteem and quality of life. Depression and other psychological disorders are more prevalent in acne patients and acne treatment may improve symptoms of these disorders. LIMITATIONS: The reviewed studies were semi-quantitative analyses utilizing various standardized surveys or questionnaires. Therefore, quantitative analysis of selected studies was not possible. CONCLUSION: The presence of co-morbid psychological disorders should be considered in the treatment of acne patients and future prospective trials are needed to assess the impact of treatment on psychological outcomes.
Introduction
Adolescence is a time of physical, emotional, and social development. Acne is a common adolescent problem, affecting more than 85 percent of teenagers, as well as some adults [1]. Although some consider acne to be merely a cosmetic problem, it may have significant and enduring emotional and psychological effects. Acne can negatively impact mood, self-esteem, and interpersonal relationships and may lead to depression and suicidal ideation [2, 3, 4]. Several studies have attempted to qualitatively and quantitatively assess the psychological effects of acne in teenagers. Here we review the current literature to determine the impact of acne on quality of life and effects on self-esteem, mood, and psychological disorders in adolescents.
Methods
 |
| Figure 1 |
|---|
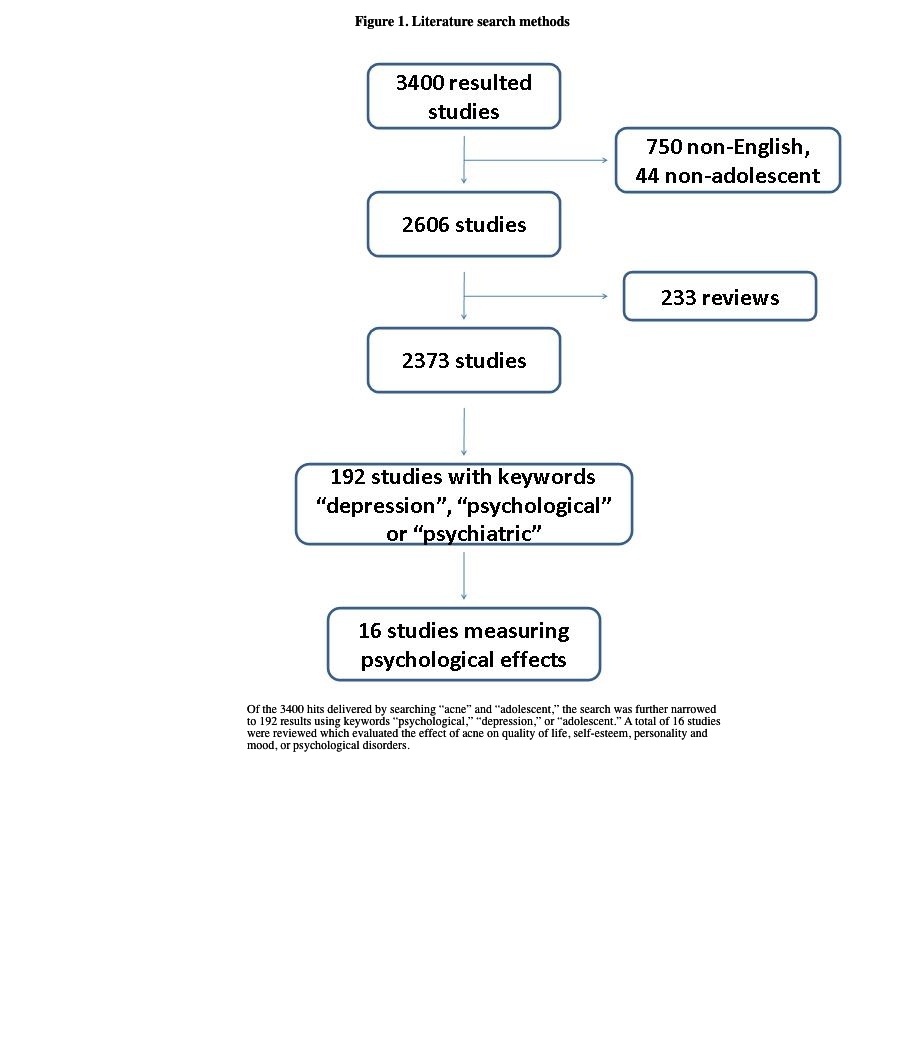
| Figure 1. Literature search methods |
A Medline search was conducted using the search terms “acne” and “adolescent” which returned 3,400 hits. Studies of adolescents, aged 13 to 18, were included for review. However, non-English language and review articles were excluded. The results were further limited using the search terms “psychological,” “depression,” and “psychiatric,” yielding 192 results. Of these, 16 studies evaluating the effect of acne on quality of life (5 studies), self-esteem (4 studies), personality and mood (2 studies), or psychological disorders (5 studies) were included for review (Figure 1). Nearly all the studies were semi-quantitative analyses of responses to surveys or standardized questionnaires. One study was a qualitative assessment of subjects’ responses to standard interview topics.
Results
Impact of acne on quality of life
A summary of all reviewed studies is presented in Table 1. Uslu et al performed a cross-sectional analysis of 600 high school students who completed the General Health Questionnaire (GHQ) and the Rosenberg Self-Esteem Scale (RSES) [5]. All participants were examined by a dermatologist who provided an objective assessment of acne severity. A total of 550 out of 600 students completed both the questionnaire and physical examination. The study population consisted of 303 girls and 260 boys, aged 13 through 19, with a mean age of 15.24. Acne was self-reported in 83.4 percent of subjects, with 40.4 percent of subjects rating their acne as mild, 36 percent moderate, and 6.5 percent severe. Self-report of acne and the dermatologist’s objective assessment were positively correlated: the prevalence of acne was 63.6 percent, with 29.2 percent non-inflammatory and 34.4 percent inflammatory acne. Acne was more prevalent and severe in boys than in girls. There was a direct correlation between subjective, but not objective, severity of acne and symptoms of anxiety, depression, and lower self-esteem based on responses to the GHQ and RSES.
A cross-sectional survey of 200 adolescents aged 15 to 18 years used two health-related quality of life questionnaires: the Children’s Dermatology Life Quality Index© (CDLQI) and the Cardiff Acne Disability Index© (CADI) [6]. Acne was reported in 83 percent of teenagers, 54 percent of males and 46 percent of females. The overall CDLQI score ranged from 0 to 19 out of a maximum 30, with a mean of 1.7 (CI -1 to 0), representing approximately 6 percent impairment. Nine subjects scored between 5 and 9, suggesting moderate (17 to 30%) impairment, whereas three scored greater than 10, suggesting severe (> 33%) impairment. Similarly, the overall CADI score ranged from 0 to 15 out of 15, with a mean of 1.9 (CI 0 to 1), representing 13 percent impairment. Twelve subjects scored between 5 and 9 (33–60% impairment), one scored 10+ (> 67% impairment), and one scored the maximum, 15 (100% impairment). There was no significant difference in mean scores between sexes for either questionnaire. The authors concluded that acne significantly impacts QOL in some teens.
Pawin et al used an adaptation of the CADI to survey 1,566 French adolescents who telephoned a youth helpline between November 2004 and January 2005 [7]. Callers were divided into those who currently had, previously had, or never had acne. Respondents included 79.4 percent females and 20.6 percent males ranging in age from 10 to 37 years, with a mean of 16.1 years. Forty-eight percent of the patients with acne indicated that their daily life was affected, which varied with the perceived acne severity (39% for mild acne, 52% for moderate acne, and 67% for severe acne; p< 0.0001). Perception of acne severity also correlated with ratings given for relationships with friends (p< 0.0001) or significant others (p< 0.0001), and with feelings of anger (p< 0.0001), sadness/anxiousness (p< 0.0001), and shame (p< 0.0001). The percentage of patients with acne who felt lonely (58.2%) or anxious (56.5%) was greater than or equal to that of patients with more serious illnesses such as diabetes, cancer, epilepsy, psychiatric disorders, and cystic fibrosis, further demonstrating the significant psychological impact of acne.
Balkrishnan et al studied 73 women, ages 17-45 (mean 37.2) with visible facial skin lesions, including acne, dermatosis papulosis, hypopigmentation, lentigines, melasma, rosacea, vascular proliferations, and other facial scars [8]. They assessed health-related quality of life (HRQOL) by Skindex-16 and fear of negative evaluation to determine whether self-perception characteristics correlated to quality of life. Fear of negative evaluation and the perception of an increased QOL without disease strongly correlated with poorer HRQOL (p< 0.05 and p< 0.01, respectively). There were no differences in HRQOL by type of facial condition. The results suggest that severe facial blemishes of any cause significantly impact women’s QOL in part through psychological effects on patients’ self-perception.
Additional measures have been proposed as a means of assessing the effect of acne on patients’ quality of life. The Acne Quality of Life Index (Acne-QOLI) is comprised of twenty-one questions about the perceived effect of acne on daily life and function [9]. The Acne-QOLI has been validated in 480 persons, ages 12 to 62 years, with mild to severe acne and has good validity, internal consistency, and test-retest reliability in the clinical setting.
Effects of acne on self-esteem
Hassan et al selected 132 patients from an acne specialist clinic and compared their responses to questionnaires including the Derriford Appearance Scale (DAS) and self-rated acne severity scales for the face, chest, and back [10]. Women had significantly greater DAS scores than men in the areas of general self-consciousness of appearance (mean score 51.3 vs. 39.7, p< 0.001), social self-consciousness (mean score 39.0 vs. 29.3, p = 0.001), sexual and bodily self-consciousness (mean score 18.0 vs. 14.0, p = 0.01), facial self-consciousness (mean score 7.4 vs. 3.9, p < 0.001), and negative self-concept (mean score 16.4 vs. 13.9, p = 0.004). Facial acne severity rating was significantly associated with social self-consciousness in women (p = 0.038) but not in men. In both men and women, back acne was associated with sexual and bodily self-consciousness of appearance (p = 0.006 and p = 0.002, respectively). The authors noted a trend for DAS scores to vary with ethnicity. Non-white men scored higher in the areas of self-consciousness of sexual and bodily appearance compared to white males and white women scored higher across all DAS subscales. However, these results did not achieve statistical significance.
A questionnaire-based survey of 3,775 tenth grade students performed in Oslo, Norway yielded an 80 percent response rate, with 13.5 percent of respondents reporting having acne [11]. The presence of acne correlated with poor self-attitude in boys alone (odds ratio 2.07, confidence interval 1.10-3.88) and poor self-worth in girls alone (odds ratio 1.88, CI 1.23-2.88). These correlations were independent of body mass index and depressive symptoms.
In another study, 26 subjects aged 13-72 with acne ranging in severity from 0.1-1.75 according to the Leeds acne grading system were interviewed using a standardized list of themed topics [12]. The authors reviewed interview transcripts, analyzing for common psychological themes among patient responses. Based on their analyses, the authors determined that patients experience immediate psychological consequences of acne including reduced self-esteem, poor self-image, self-consciousness and embarrassment. The effects were common to both men and women and were exacerbated by taunting, stigmatization, and perceptions of scrutiny and being judged. Acne had a permanent effect on the personality and behavior of older subjects, causing them to avoid interaction and social situations, as is common in persons with social phobias or avoidant personality disorder.
Smithard et al surveyed 317 students using an age-appropriate Strengths and Difficulties Questionnaire (SDQ) and an Acne Management Questionnaire to assess psychological health, level of acne knowledge and help-seeking behavior [13]. Acne severity was graded using an adapted form of the Leeds acne grading scale. The study was comprised of 153 boys (48%) and 164 girls (52%), aged 14-16 years. Seventy-seven percent of participants scored within the normal range of the SDQ, with 52 children (16%) classified as “borderline abnormal” and 22 (7%) as “probably abnormal.” Approximately half had acne (53% boys and 45% girls), with 11 percent of participants having moderate to severe acne. Female students and those who had definite acne, defined as more than 12 lesions, had significantly higher levels of emotional and behavioral difficulties based on SDQ score (p< 0.05 and p< 0.01, respectively). Participants with acne were nearly twice as likely as those without acne to score in the abnormal/borderline range of the SDQ (32% vs. 20%; odds ratio 1.86, 95% CI 1.03-3.34). Although the response rate was adequate, 20 percent of pupils refused to take part in or were absent during the study. The authors suggest that this could represent more vulnerable teenagers or those most embarrassed by their skin and this study would then underestimate the psychological effects of acne.
Effects of acne on personality and mood
Trait anger, the disposition to experience angry feelings as a personality trait, has been associated with heart disease and other morbidities. Rapp et al analyzed the association of acne with trait anger (TA) and its impact on quality of life [14]. The authors surveyed 479 subjects and compared respondents who reported high TA to those with low TA on outcome variables. High TA was inversely correlated with global quality of life (p< 0.001), skin-related quality of life (p< 0.002), satisfaction with treatment (p = 0.001) and adherence to treatment advice (p< 0.05) in bivariate analyses. However, there was no difference in acne severity between subjects with high or low TA (p = 0.2). The results suggest that emotional states, such as anger, may impact the quality of patients’ lives and satisfaction with treatment, and should be considered in the care of acne patients.
Krejci-Manwaring et al analyzed the association of the personality trait of dispositional social sensitivity and the adverse social impact of acne [15]. Four hundred seventy-nine subjects with acne aged 16-62 were surveyed and classified as having either high or low social sensitivity. Demographic characteristics, acne characteristics, and quality of life were also assessed. There was a positive correlation between acne severity and poorer social outcomes and quality of life (p< 0.05). For women, higher social sensitivity was independently associated with poorer outcomes (p< 0.05), whereas for men, higher social sensitivity correlated with acne severity and was associated with worse social outcomes and life quality (p< 0.05). The authors concluded that dispositional social sensitivity in acne patients was independently associated with poorer social functioning and quality of life.
Acne and psychological disorders
In addition to its negative impact on self-esteem and mood, acne is associated with anxiety, depression and suicidal ideation, and other psychological disorders. Purvis et al performed a secondary analysis of a 2001 national health and well-being survey administered to 9,567 secondary school students in New Zealand aged 12 to 18 [16]. Outcomes measured included self-reported acne, depressive symptoms, anxiety, and self-reported suicide attempts. The overall response rate was 64.3 percent, representing 4 percent of the total number of students in New Zealand secondary schools. Fourteen percent of students reported having “problem acne.” Symptoms of clinically relevant depression were reported by 1,294 (14.1%) students and 432 (4.8%) reported symptoms of anxiety. The presence of depressive symptoms had a positive correlation with increasing acne severity. More than 2,000 students (23.6%) reported having suicidal thoughts and 730 (7.8%) reported a prior suicide attempt in the last 12 months. Problem acne was associated with an increase in frequency of suicidal thoughts and suicide attempts. The association between problem acne and suicide attempts persisted when the authors controlled for depressive symptoms and anxiety (odds ratio 1.50, 95% CI 1.21-1.86).
Uhlenhake et al conducted a retrospective examination of patient information from a medical claims database using the Total Resource Utilization Benchmarks™, which included age, gender, co-morbid depression, antidepressant utilization, and acne treatment modality [17]. Clinical depression was present in 8.8 percent of acne patients; this was 3 to 4 times greater than the prevalence of depression in the general population. Sixty-five percent of acne patients were female; twice as many females were reported to have depression than males (10.6% females vs. 5.3% males). The analysis only included patients who had sought treatment for their acne and also reported having clinical depression. Therefore it may have underestimated the total prevalence of acne and associated depression in the general population.
The prevalence of Body Dysmorphic Disorder (BDD), in which the affected person is excessively concerned about a perceived defect in his or her physical features, was also examined among acne patients [18]. The study was based on responses of 128 subjects to a self-reporting questionnaire and objective assessments of acne severity by a single observer. Rates of BDD ranged from 14.1 to 21.1 percent, depending on the stringency of criteria used. The risk of BDD was increased by two-fold in patients requiring systemic isotretinoin therapy.
Isotretinoin therapy is used in the treatment of severe or recalcitrant acne. Several case reports have raised concern over the increased incidence of depression and suicide in patients receiving isotretinoin therapy (for review see Jacobs et al 2001) [19]. A case-crossover study analyzed 126 patients receiving isotretinoin therapy who had received a diagnosis of depression or who were hospitalized for depression from 1984-2003 [20]. The study demonstrated a statistically significant association between isotretinoin and depression with a relative risk of 2.00 (95% CI 1.03 to 3.89) in isotretinoin-exposed patients. The adjusted relative risk was 2.68 (95% CI 1.10 to 6.48) after controlling for potential time-dependent confounders.
In contrast, a prospective cohort study compared 100 patients receiving isotretinoin therapy to 41 patients receiving topical and 59 receiving oral antibiotic therapy for acne [21]. Depression was assessed at baseline and 2 months after therapy, using the Center for Epidemiologic Studies Depression scale and the Zung Depression Status Inventory. No association between isotretinoin and the development of depression was noted.
Marqueling et al performed a review of nine studies analyzing depression and suicidal ideation in patients treated with isotretinoin [22]. No increase was observed in the incidence of depression diagnoses or depressive symptoms following treatment. In fact, some studies demonstrated a trend toward fewer or less severe depressive symptoms after isotretinoin therapy, particularly in those patients with moderate or clinical depression prior to treatment. Furthermore, there was no correlation between isotretinoin use and suicidal behavior. The authors concluded that the available data on suicidal behavior during isotretinoin therapy are insufficient to establish a causative association.
Treatment with isotretinoin is also associated with improved quality of life. Hahm et al conducted a cohort study of 38 acne patients who were started on isotretinoin therapy [23]. Patients were examined before initiation of therapy and at weeks 2 and 8. Study subjects showed improvement in acne severity and overall quality of life after 8 weeks, assessed by the Leeds revised acne grading system and the Assessment of the Psychological and Social Effects of Acne (APSEA). Depressive severity decreased within 2 weeks of starting isotretinoin therapy. There was a significant correlation between depression, graded by the Beck depression inventory (BDI) scale, and quality of life by APSEA, but no association between BDI and acne severity.
Kaymak et al analyzed 78 patients randomized to isotretinoin or topical treatment [24]. Psychological status was evaluated at baseline and at 2 and 4 months by patient responses to the dermatology life quality index (DLQI), the hospital anxiety and depression (HAD) scale, and the BDI. At the end of the second month, quality of life was significantly poorer in patients receiving topical treatment compared to isotretinoin therapy (p< 0.05). However, there was no difference in the HAD or BDI scores between the two groups. The results suggest that there is no increase in depressive or anxiety symptoms in patients receiving isotretinoin therapy and are consistent with previous studies showing no correlation between isotretinoin therapy and depression or suicidal behavior [25, 26, 27, 28]. However, this does not exclude the possibility that isotretinoin may cause or exacerbate depression in some patients [29] and patients should be monitored for symptoms of depression.
Conclusion
The presence of acne can negatively affect quality of life, self-esteem, and mood in adolescents. Acne is associated with an increased incidence of anxiety, depression, and suicidal ideation. The presence of these and other co-morbid psychological disorders should be considered in the treatment of acne patients when appropriate. A strong physician-patient relationship and thorough history taking may help to identify patients at risk for the adverse psychological effects of acne. Successful treatment of acne with isotretinoin qualitatively decreases depressive symptoms and improves quality of life. The effect of other topical and systemic therapies for acne on psychological symptoms has not been assessed.
In addition to the effect of acne on the patient, family and social relationships may also be strained. Parents may worry about the short- and long-term repercussions of their child’s appearance, such as being bullied at school or having permanent scarring from acne lesions. As teens gain independence during adolescence, their attitudes toward treatment and adherence to the prescribed regimen may be adversely affected. Parents and patients may not always be adequately educated about the causes and treatment of acne, which may further delay or affect successful treatment [30]. Poor adherence to therapy is a barrier to successful acne treatment. There is a positive correlation between treatment adherence and improved quality of life for other cutaneous diseases such as psoriasis [31, 32] and is an important area of future research in the clinical setting of acne treatment.
One limitation of the presented studies is that the majority are qualitative, questionnaire-based, case-controlled, or cross-sectional studies, which may introduce bias associated with self-reporting. The questionnaires used are appropriate as screening tools to assess for underlying psychological disorders, but are not sufficient to diagnose clinical depression or anxiety. Future prospective trials may help to more clearly define the psychological effects of acne on patients and their families and determine whether anti-acne therapy is successful in improving these parameters.
References
1. Balkrishnan R, Kulkarni AS, Cayce K, et al. Predictors of healthcare outcomes and costs related to medication use in patients with acne in the United States. Cutis 2006 Apr;77(4):251-5. [PubMed]2. Ayer J, Burrows N. Acne: more than skin deep. Postgrad Med J 2006 Aug;82(970):500-6. [PubMed]
3. Fried RG, Gupta MA, Gupta AK. Depression and skin disease. Dermatol Clin 2005 Oct;23(4):657-64. [PubMed]
4. Fried RG, Wechsler A. Psychological problems in the acne patient. Dermatol Ther 2006 Jul;19(4):237-40. [PubMed]
5. Uslu G, Sendur N, Uslu M, et al. Acne: prevalence, perceptions and effects on psychological health among adolescents in Aydin, Turkey. J Eur Acad Dermatol Venereol 2008 Apr;22(4):462-9. [PubMed]
6. Walker N, Lewis-Jones MS. Quality of life and acne in Scottish adolescent schoolchildren: use of the Children's Dermatology Life Quality Index (CDLQI) and the Cardiff Acne Disability Index (CADI). J Eur Acad Dermatol Venereol 2006 Jan;20(1):45-50. [PubMed]
7. Pawin H, Chivot M, Beylot C, et al. Living with acne. A study of adolescents' personal experiences. Dermatology 2007;215(4):308-14. [PubMed]
8. Balkrishnan R, McMichael AJ, Hu JY, et al. Correlates of health-related quality of life in women with severe facial blemishes. Int J Dermatol 2006 Feb;45(2):111-5. [PubMed]
9. Rapp SR, Feldman SR, Graham G, et al. The Acne Quality of Life Index (Acne-QOLI): development and validation of a brief instrument. Am J Clin Dermatol 2006;7(3):185-92. [PubMed]
10. Hassan J, Grogan S, Clark-Carter D, et al. The individual health burden of acne: appearance-related distress in male and female adolescents and adults with back, chest and facial acne. J Health Psychol 2009 Nov;14(8):1105-18. [PubMed]
11. Dalgard F, Gieler U, Holm JO, et al. Self-esteem and body satisfaction among late adolescents with acne: results from a population survey. J Am Acad Dermatol 2008 Nov;59(5):746-51. [PubMed]
12. Magin P, Adams J, Heading G, et al. Psychological sequelae of acne vulgaris: results of a qualitative study. Can Fam Physician 2006 Aug;52:978-9. [PubMed]
13. Smithard A, Glazebrook C, Williams HC. Acne prevalence, knowledge about acne and psychological morbidity in mid-adolescence: a community-based study. Br J Dermatol 2001 Aug;145(2):274-9. [PubMed]
14. Rapp DA, Brenes GA, Feldman SR, et al. Anger and acne: implications for quality of life, patient satisfaction and clinical care. Br J Dermatol 2004 Jul;151(1):183-9. [PubMed]
15. Krejci-Manwaring J, Kerchner K, Feldman SR, et al. Social sensitivity and acne: the role of personality in negative social consequences and quality of life. Int J Psychiatry Med 2006;36(1):121-30. [PubMed]
16. Purvis D, Robinson E, Merry S, et al. Acne, anxiety, depression and suicide in teenagers: a cross-sectional survey of New Zealand secondary school students. J Paediatr Child Health 2006 Dec;42(12):793-6. [PubMed]
17. Uhlenhake E, Yentzer BA, Feldman SR. Acne vulgaris and depression: a retrospective examination. J Cosmetic Dermatol 2010;9:59-63
18. Bowe WP, Leyden JJ, Crerand CE, et al. Body dysmorphic disorder symptoms among patients with acne vulgaris. J Am Acad Dermatol 2007 Aug;57(2):222-30. [PubMed]
19. Jacobs DG, Deutsch NL, Brewer M. Suicide, depression, and isotretinoin: is there a causal link? J Am Acad Dermatol 2001 Nov;45(5):S168-S175. [PubMed]
20. Azoulay L, Blais L, Koren G, et al. Isotretinoin and the risk of depression in patients with acne vulgaris: a case-crossover study. J Clin Psychiatry 2008 Apr;69(4):526-32. [PubMed]
21. Cohen J, Adams S, Patten S. No association found between patients receiving isotretinoin for acne and the development of depression in a Canadian prospective cohort. Can J Clin Pharmacol 2007;14(2):e227-e233. [PubMed]
22. Marqueling AL, Zane LT. Depression and suicidal behavior in acne patients treated with isotretinoin: a systematic review. Semin Cutan Med Surg 2007 Dec;26(4):210-20. [PubMed]
23. Hahm BJ, Min SU, Yoon MY, et al. Changes of psychiatric parameters and their relationships by oral isotretinoin in acne patients. J Dermatol 2009 May;36(5):255-61. [PubMed]
24. Kaymak Y, Taner E, Taner Y. Comparison of depression, anxiety and life quality in acne vulgaris patients who were treated with either isotretinoin or topical agents. Int J Dermatol 2009 Jan;48(1):41-6. [PubMed]
25. Simic D, Situm M, Letica E, et al. Psychological impact of isotretinoin treatment in patients with moderate and severe acne. Coll Antropol 2009 Dec;33 Suppl 2:15-9. [PubMed]
26. Marqueling AL, Zane LT. Depression and suicidal behavior in acne patients treated with isotretinoin: a systematic review. Semin Cutan Med Surg 2005 Jun;24(2):92-102. [PubMed]
27. Jick SS, Kremers HM, Vasilakis-Scaramozza C. Isotretinoin use and risk of depression, psychotic symptoms, suicide, and attempted suicide. Arch Dermatol 2000 Oct;136(10):1231-6. [PubMed]
28. Chia CY, Lane W, Chibnall J, et al. Isotretinoin therapy and mood changes in adolescents with moderate to severe acne: a cohort study. Arch Dermatol 2005 May;141(5):557-60. [PubMed]
29. Hull PR, D'Arcy C. Isotretinoin use and subsequent depression and suicide: presenting the evidence. Am J Clin Dermatol 2003;4(7):493-505. [PubMed]
30. Tan JK, Vasey K, Fung KY. Beliefs and perceptions of patients with acne. J Am Acad Dermatol 2001 Mar;44(3):439-45. [PubMed]
31. Zaghloul SS, Goodfield MJ. Objective assessment of compliance with psoriasis treatment. Arch Dermatol 2004 Apr;140(4):408-14. [PubMed]
32. Renzi C, Picardi A, Abeni D, et al. Association of dissatisfaction with care and psychiatric morbidity with poor treatment compliance. Arch Dermatol 2002 Mar;138(3):337-42. [PubMed]
© 2011 Dermatology Online Journal