Eruptive syringomas
Published Web Location
https://doi.org/10.5070/D34bt5t2xkMain Content
Eruptive syringomas
Marta Teixeira, Márcia Ferreira, Susana Machado, Rosário Alves, and Manuela Selores
Dermatology Online Journal 11 (3): 34
Dermatology Department, Hospital Geral de Santo António, Porto, Portugal. martamotateixeira@mail.telepac.pt
Abstract
Eruptive syringoma is a rare clinical presentation of a benign tumor of the eccrine ducts. It consists in successive crops of small skin-colored papules on the anterior body surfaces. It generally occurs in the peri-pubertal period. Treatment of this benign condition is cosmetic only. A case of a 19-year-old female with a 5-year history of eruptive syringoma is presented.
Clinical synopsis
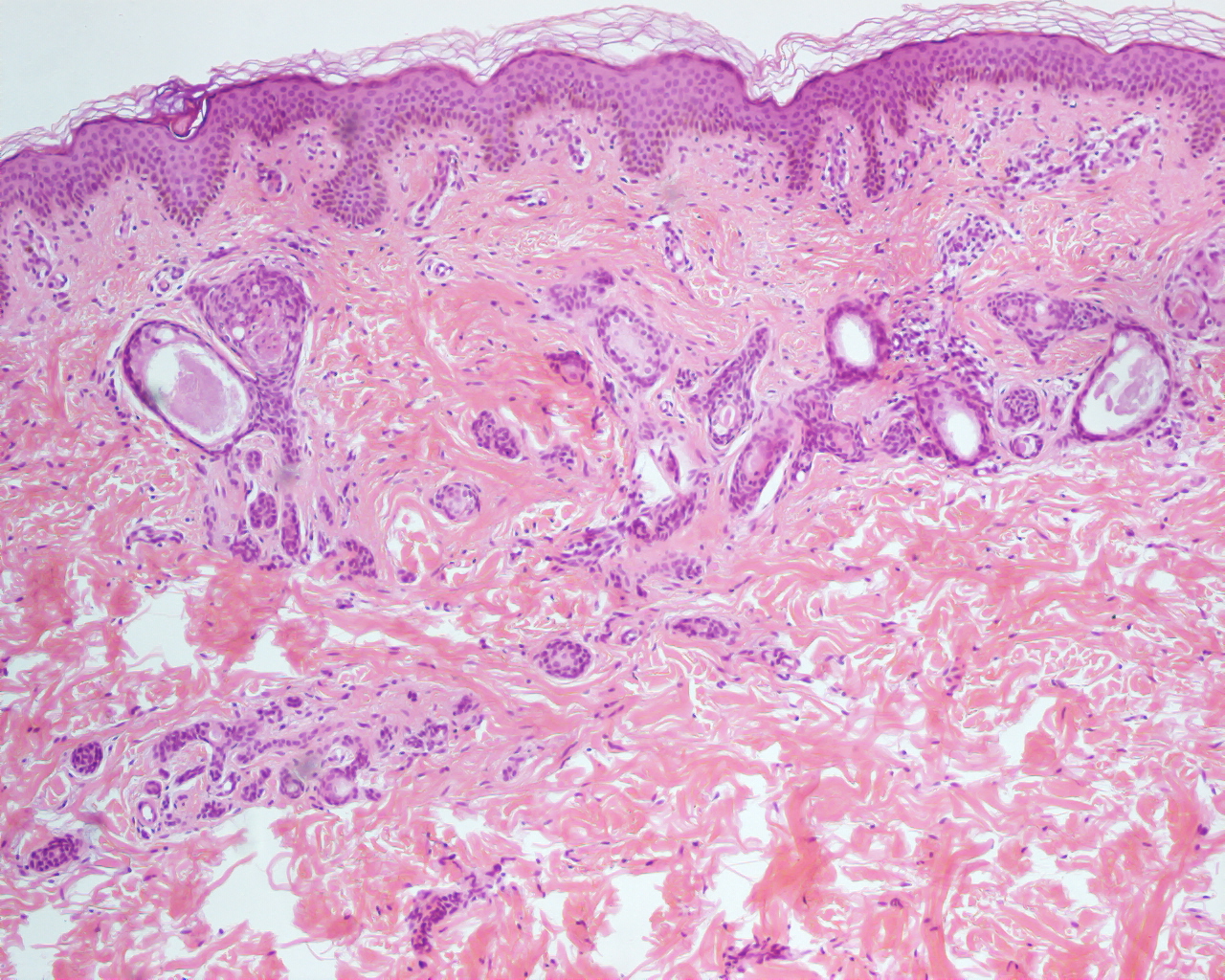
A 19-year-old, healthy, white female presented with a 5-year history of eruptions that began as a few papules on the anterior chest wall and spread to a larger area on her upper body in successive crops. The lesions were asymptomatic and, since they first appeared, the patient's skin had never been completely clear. She was not on any medication, no family member had ever had a similar skin condition, and review of systems was noncontributory. Physical examination revealed multiple, skin- to tan-colored, flat-topped papules 1 to 3 mm in diameter on the neck, shoulders, anterior chest, abdomen and axillae (Figs. 1 and 2). The lesions were bilateral, symmetrical, and had both a follicular and nonfollicular distribution. No puncta or significant surface changes were noted and Darier sign was negative. The remainder of the physical examination was unremarkable. A skin biopsy was obtained from a lesion in the neck (Figs. 3 and 4). Punch biopsy specimen revealed a normal epidermis overlying a dermis that was filled with multiple ducts embedded in a fibrous stroma. The ducts were lined by an inner layer of flattened epithelial cells. Some had a tadpole like appearance due to the presence of a comma-like tail that was formed by cells projecting from one side of the duct into the stroma (Fig. 3). Ductal lumina were filled with an amorphous, periodic acid-Schiff-positive material (Fig. 4).

|

|
| Figure 1 | Figure 2 |
|---|---|
| Multiple skin- to tan-colored flat-topped papules on the axillae, neck, and anterior chest. | |

|
|
| Figure 3 | Figure 4 |
|---|---|
| Figure 3. Hematoxilin-eosin stained section showing collections of cystic ducts and some epithelial cords with comma-like tails (x10). | |
| Figure 4. Ductal lumina filled with an amorphous periodic acid-Schiff-positive material (x20). | |
Discussion
Syringoma is a benign adnexal tumor that derives from the intraepidermal portion of eccrine sweat ducts. Syringomas appear during puberty or the third or fourth decade [1, 2, 3]. Although the variety localized on the eyelid in middle-aged women is the most frequent, many other clinical variants are reported. Friedman and Butler proposed a classification according to clinical features and associations. This consisted of four principal clinical variants of syringoma: a localized form, a familial form, a form associated with Down syndrome, and a generalized form that encompasses multiple and eruptive syringoma [3].
Lesions are more common in women than men, in Japanese people, and patients with Down syndrome [1, 2]. Patients with diabetes mellitus may present with a histological variant known as clear-cell syringoma [4]. In one reported case, it was associated with carcinoid tumor [5].
In eruptive syringoma, a rare variant first described by Jacquet and Darier in 1987, the lesions occur in large numbers and in successive crops on the anterior chest, neck, upper abdomen, axillae, and periumbilical region at puberty or during childhood [6]. More rarely cases with wider involvement of the body have also been reported. It occurs more frequently among women. The lesions consist of asymptomatic multiple small firm yellow-brown-colored papules, that typically present in a bilateral, symmetrical distribution, but there have been reports of unilateral, unilateral nevoid, bathing trunk and generalized distributions [1, 2]. Clinically, it may be mistaken for acne vulgaris, sebaceous hyperplasia, milia, lichen planus, eruptive xanthoma, urticaria pigmentosa, or hidrocystoma. Definitive diagnosis can be made on histological examination, because syringomas demonstrate distinctive histophatological features. Examination of the dermis demonstrates numerous, small ducts lined with a double row of flattened epithelial cells. Often the outer layer extends into the surrounding stroma, forming a comma-like projection. Ductal lumina are filled with an amorphous, periodic acid-Schiff-positive material. Histochemical and electron microscopic findings have confirmed that syringomas represent adenomas of eccrine sweat ducts [7].
Treatment of syringoma is cosmetic. Therefore it should not be confused with the above referred differential diagnosis. Options are abundant and generally unsatisfactory. Treatment modalities have included dermabrasion, various methods of excision, cryosurgery, electrodesiccation, chemical peeling and oral and topical retinoids [8, 9, 10]. Successful treatment of facial syringomas with carbon dioxide laser also has been reported [11]. A recent report suggests the use of topical atropine to alleviate the pruritus in symptomatic eruptive syringoma [12]. Because they are located in the dermis and often numerous, unfortunately, there is no standard treatment for widespread syringomas, as in our patient. Any method of surgical or chemical destruction carries the risk of scarring. Furthermore, none eliminates the risk of recurrence. Rarely, tumors may regress spontaneously in adulthood [1, 2, 8, 9, 10, 11, 12].
References
1. Patrizi A, Neri I, Marzaduri S, et al. Syringoma: a review of twenty-nine cases. Acta Derm Venereol (Stockh). 1998;78:460-4622. Soler-Carrilo J, Estrach T, Mascaró JM. Eruptive syringoma: 27 new cases and review of the literature. J Eur Acad Dermatol Venereol. 2001;15:242-246
3. Friedman SJ, Butler DF. Syringoma presenting as milia. J Am Acad Dermatol. 1987;16:310-314
4. AmbrojoP, Requena Caballero L, Aguilar Martinez L, et al. Clear-cell syringoma: microscopy study. Dermatologica. 1989;178:164-166
5. Berbis P, Fabre JF, Jancovic E, et al. Late-onset syringomas of the upper extremities associated with carcinoid tumor. Arch Dermatol Venereol. 1989;125:848-849
6. Jacquet L, Darier J. Hiydradénomes éruptifs, épithéliomes adénoides des glandes sudoripares ou adénomes sudoripares. Ann Dermatol Syph. 1887 ;8:317-323
7. Goyal S, Martins CR. Multiple syringomas on the abdomen, thighs and groin. Cutis. 200;66:259-262
8. Karam P, Benedetto AD. Syringomas: new approach to an old technique. Int J Dermatol. 1996;35:219-220
9. Janninger CK, Brodkin RH. Eruptive syringomas. Cutis. 1990;46:427-429
10. Gomez MI, Prez B, Azana JM, et al. Eruptive syringoma: treatment with topical tretinoin. Dermatology. 1994;189:105-106
11. Wang JI, Roening HH Jr. Treatment of multiple facial syringomas with carbon dioxide (CO2) laser. Dermatol Surg. 1999;25:136-139
12. Sánchez TS, Daudén E. Eruptive pruritic syringomas: treatment with topical atropin. J Am Acad Dermatol.2001;44:148-149 [Letter]
© 2005 Dermatology Online Journal