Preradial myxedema in a euthyroid male: A distinct rarity

Main Content
Preradial myxedema in a euthyroid male: A distinct rarity
Shyam Verma1 DVD FRCP, Franco Rongioletti2 MD, Markus Braun-Falco3 MD, Thomas Ruzicka3 MD
Dermatology Online Journal 19 (4): 9
1. Nirvana Skin Clinic, Vadodara, Gujarat, India2. Department of Dermatology, University of Genoa, Italy
3. Department of Dermatology, University of Munich, Munich, Germany
Abstract
Localized or pretibial myxedema is one of the signs of Graves disease (along with goiter, exophthalmus, thyroid acropathy, and high circulating levels of long-acting thyroid-stimulating hormone) and usually tends to occur at a later stage of the disease or even after the patient becomes euthyroid post treatment. Very rarely has it been reported in euthyroid patients. We report a euthyroid man presenting with localized myxedema on the extensor surface of his forearm with clinical and histopathological features consistent with pretibial myxedema. He responded partially to topical clobetasol propionate cream and tacrolimus ointment 0.1 percent for about 7 months. To the best of our knowledge, this is the first case of preradial myxedema in a euthyroid patient in the English international dermatological literature
Introduction
Primary cutaneous mucinosis can present in many forms. When it presents on the lower legs in patients with underlying thyroid disorders it is called pretibial myxedema. A 72-year-old patient is being reported with a localized skin colored plaque with peau d’orange appearance, which was initially treated as leprosy. Upon biopsy it showed a mucinous deposit characteristic of pretibial myxedema. The patient was extensively investigated and no thyroid abnormality was found. Clincopathologic correlation allowed a diagnosis of preradial myxedema in a euthyroid patient. This is the first time such a case is being reported in international literature.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. (1A) Preradial skin-colored, waxy indurated plaque with accentuated follicular openings giving it a classical peau
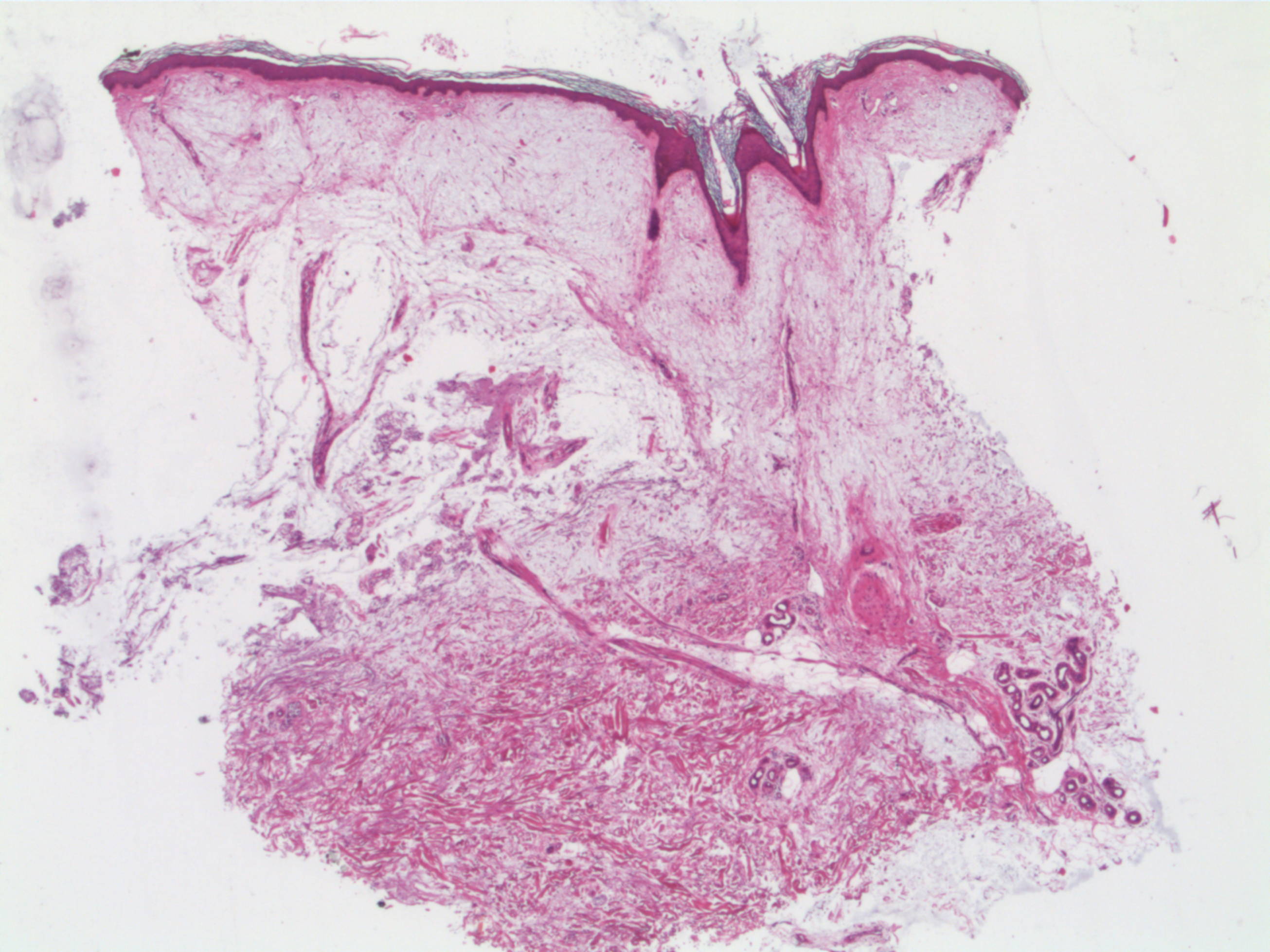
de orange appearance. (1B) Close-up of the plaque on the preradial area. Figure 2. Large quantities of mucin are deposited in the reticular dermis, causing collagen bundles to separate and the dermis to thicken. A grenz zone of normal collagen is also observed as well as orthohyperkeratosis, follicular plugging, and acanthosis (H&E x2.5). | |
A 72-year-old man presented to this clinic with a large swelling on the right forearm for the past 2 years. He had developed this gradually and about three months prior to presentation he had gone to a private dermatologist who had diagnosed it as leprosy and had started treatment. On examination the patient had a large plaque extending from the wrist to the elbow involving the entire extensor surface of the forearm and also extending to the medial surface in parts. The surface of the plaque had accentuated follicular openings giving it a classical peau de orange appearance (Figures 1 and 2). It was firm on palpation and freely movable. The plaque seemed to have less hair when compared with the other forearm. There was no sensory deficit. There were no palpable nerves leading to the patch and all other peripheral nerves were normal. No other body area was affected. His blood count, blood sugar, ANA, and serum immunoglobulins were normal. X-ray chest and USG abdomen did not show anything abnormal. His T3, T4 and TSH, antiperoxidase, antithryroglobulin, and anti TSH receptor antibodies were normal. USG of thyroid gland did not reveal any abnormality. Ophthalmic examination was normal.
 |  |
| Figure 3 | Figure 4 |
|---|---|
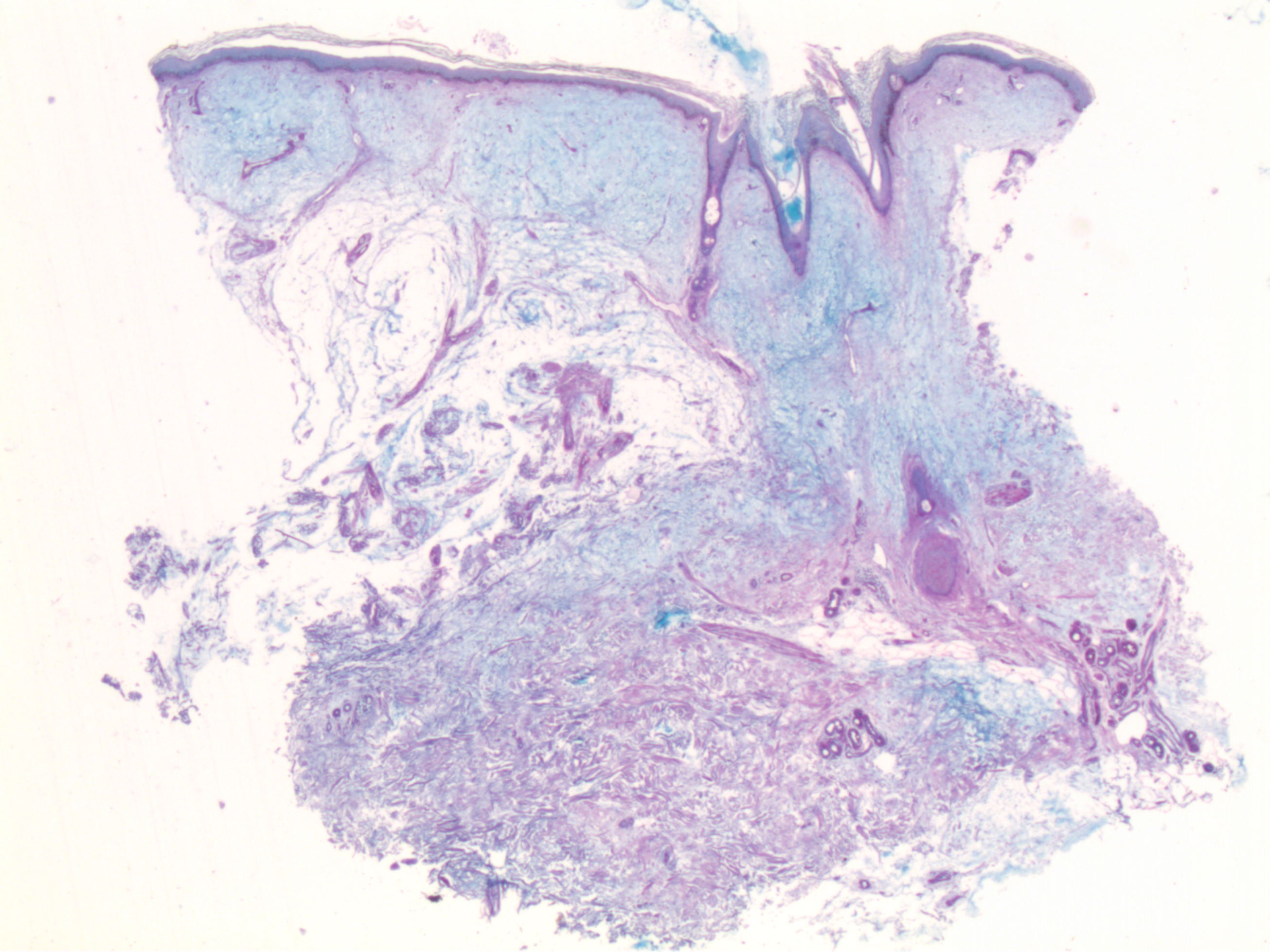
| Figure 3. Same findings in (Alcian Blue 2.5% x2.5) Figure 4. Notable flattening of the lesion after clobetasol and tacrolimus ointments | |
A 4 mm punch biopsy yielded skin with a distinctly gelatinous appearance and consistency. A mucinous pathology was suspected. Histological examination showed a basket weave thickened stratum corneum with follicular hyperkeratosis and acanthosis. Focal areas of thinned out epidermis with flattening of rete ridges owing to the pressure of the underlying mucin were also seen. There was a large diffuse deposition of mucin throughout the reticular dermis with attenuation of collagen fibers, sparing a subtle band in the papillary dermis (Figure 3). The fibers were frayed, fragmented, and widely separated owing to the extensive deposition of mucin. The spindle shaped and stellate fibroblasts appeared to float in the edematous areas but the number was not largely increased. There were no increased mast cells. The clinicopathological correlation allowed the diagnosis of localized myxedema in a euthyroid patient. He was prescribed topical clobetasol propionate cream and tacrolimus ointment 0.1 percent, which he applied very erratically. After discussing this issue in a follow up visit he began to regularly apply the medication for 7 months and showed significant flattening of the lesion (Figure 4).
Discussion
Cutaneous mucinoses are a heterogenous group of disorders in which there is deposition of abnormal amounts of mucin in the skin. This group of disorders is broadly divided into distinctive mucinoses (primary) in which deposition of mucin is the hallmark resulting in characteristic clinical lesions and secondary mucinoses in which mucin is found histologically as an additional finding [1]. The first group of primary mucinoses is divided into two subgroups, degenerative-inflammatory mucinoses and neoplastic hamartomatous mucinoses. The former may be dermal or follicular. Mucin is a normal constituent of many organs of the body including the skin. It is amorphous and gelatinous in consistency and its main component is hyaluronic acid. There are two types of mucin, dermal and epithelial. Dermal mucin is produced by fibroblasts in small amounts and is found in the ground substance of the dermis [1, 2]. It is PAS negative and stains with alcian blue at pH 2.5 but not at pH 0.4 [1, 2]. It is difficult to diagnose the various clinical variations of dermal mucinoses; the diagnosis rests mainly on clinicopathological correlation (Table 1). Three histologic clues include the pattern of mucin distribution, focal or diffuse, the level of deposit in the dermis, upper or lower, and additional findings [1].
We report a rare and interesting presentation of a primary cutaneous mucinosis presenting as a solitary plaque on the forearm with a peau de orange appearance characteristic of localized myxedema in the preradial area. The well-defined plaque with accentuated hair follicles can be explained by the large amounts of mucin underlying the epidermis. The relative alopecia in this particular plaque could be attributed to vigorous massaging with vegetable oil by the patient. The initial clinical diagnosis of leprosy was not tenable on clinical nor histological grounds.
Had this plaque appeared on the pretibial area in a patient with hyperthyroidism it would have been undoubtedly labeled as a classic case of pretibial myxedema. Localized myxedema is most commonly described in patients with hyperthyroidism, especially Graves disease. It can however also occur after a patient has undergone radioactive iodine treatment or thyroid surgery, in which case it is also known to regress spontaneously [2]. It can also present in the absence of hyperthyroidism, when the patient begins to be treated for acute hyperthyroidism, or after treatment has resulted in a hypothyroid or euthyroid state [2]. Although pretibial myxedema generally appears as indurated plaques on the shins it has also been rarely reported in other areas such as the face, shoulders, arms, and abdomen [2-6]. Thickening of the extensor aspect of the skin of the forearms has been demonstrated in patients with Graves disease. These have also demonstrated collections of mucin leading to the author's suggesting that preradial myxedema is a counterpart of pretibial myxedema [3]. Finally, very rarely pretibial myxedema has been reported in euthyroid patients [7, 8].
Localized myxedema is characterized by large amounts of mucin in the interstitium of the dermis, especially in the upper half leading to a thickened dermis. This also causes wide separation of collagen bundles [1, 9]. Elastic fibers are usually decreased. The fibroblasts are not increased in number but may be stellate [9]. Hyperkeratosis and follicular plugging are more prominent than seen in generalized myxedema. Our patient had classic histologic features of localized myxedema [1, 9].
It appears logical to treat preradial myxedema similarly to pretibial myxedema because there are no guidelines to treat the former owing to its rarity. No natural history of the disease is studied but resolution of lesions has been reported on an average after 42 months in one study [2]. Complete remission occurs in about 25 percent of cases [9, 10]. Although it is not clear how steroids work in localized myxedema, oral corticosteroids, topical corticosteroids under occlusion, and intralesional corticosteroids have been used with varying success [10]. Topical tacrolimus and surgical debulking have also been described to be successful in isolated cases. Our patient showed partial flattening of the lesion after 7 months of application of tacrolimus and clobetasol propionate.
In conclusion we report an intriguing and unusual case of preradial myxedema in a euthyroid patient with a characteristic histology, which we believe is the first case in the dermatological literature. We plan to follow this patient to see if he shows signs of dysthyroidism at some time in the future.
Learning Points
- Cutaneous mucinosis is a large family of depositional disorders in which mucin is seen in large amounts either primarily or secondarily.
- A peau de orange asymptomatic plaque on the forearm can be mistaken for tuberculoid leprosy in an endemic country as was seen in this case.
- A mucinous pathology was seen in the biopsy, which was identical to what has been described in pretibial myxedema.
- Considering there are rare cases of localized myxedema reported on sites other than the legs this was considered to be a rare case of preradial myxedema.
- Myxedema is associated with thyroid disorders, but in this case T3, T4 and TSH, antiperoxidase, antithryroglobulin, and anti TSH receptor antibodies were all negative; ultrasonography of the thyroid gland was normal.
- This appears to be the first case of preradial myxedema in a euthyroid patient.
- The patient responded to topical clobetasol and tacrolimus ointment.
References
1. Rongioletti F, Rebora A. Cutaneous mucinoses: microscopic criteria for diagnosis. Am J Dermatopathol. 2001 Jun;23(3):257-67. [PubMed]2. Truhan AP, Roenigk HH Jr The cutaneous mucinoses. J Am Acad Dermatol. 1986 Jan;14(1):1-18. [PubMed]
3. Wortsman J. Dietrich J, Traycoff RB, et al: Preradial myxedema in thyroid disease. Arch Dermatol 117:635-638, 1981 [PubMed]
4. Noppakun N, Bancheun K, Chandraprasert S. Unusual locations of localized myxedema in Graves' disease. Report of three cases. Arch Dermatol. 1986 Jan;122(1):85-8. [PubMed]
5. Cohen BD, Benna RS, Rawson RW: Localized myxedema involving the upper extremities. Arch Intern Med 111:641-646, 1963. [PubMed]
6. Perry HO, Kierkland RR, Montgomery H. Plaque-like form of cutaneous mucinosis. Arch Dermatol. 1960 Dec;82:980-5 [PubMed]
7. Buljan-Cvijanovic M, Neal JM, Zemtsov A. Euthyroid pretibial myxedema. Endocr Pract. 1998;4:375-377 [PubMed]
8. Srebrnik A, Ophir J, Brenner S. Euthyroid pretibial myxedema. Int J Dermatol. 1992;31:431-2. [PubMed]
9. Lever’s Histopathology of the skin. Elder DE. 10th ed. Lippincot & Wilkins 2009. 10th ed.
© 2013 Dermatology Online Journal