Type II lepra reaction: An unusual presentation
Published Web Location
https://doi.org/10.5070/D3448655c6Main Content
Type II lepra reaction: An unusual presentation
S Chauhan MD1, S D'Cruz MD DM1, H Mohan MD2, R Singh MD1, J Ram MD1, A Sachdev MD DM1
Dermatology Online Journal 12 (1): 18
Departments of Medicine1 and Pathology 2, Government Medical College and Hospital, Sector 32, Chandigarh, India. drsc88@rediffmail.comAbstract
Ulcers with maculo-papular rash are an unusual presenting feature of leprosy. They occur as result of neuropathy, type-2 lepra reaction or Lucio's phenomenon. The hall mark of type-2 reaction is erythema nodosum. Very rarely it manifests as ulcerative skin lesions. We describe one such unusual case of a young male who presented with multiple ulcers and maculo-papular rash over the legs, chest and abdomen. In addition to this, he had fever, heart murmur, pulmonary infiltrates, neuropathy, and elevated liver enzymes. A clinical differential diagnosis of infective endocarditis or systemic nectrozing vasculitis was considered. Skin biopsy showed dense inflammation with lepra bacilli consistent with type-2 lepra reaction.
Introduction
Leprosy is a multi-organ infectious disease affecting mainly the skin and the nerves. Leprosy is also associated with type-1 and type-2 reactions [1]. Ulcers are an uncommon presentation of leprosy. These occur as a result of loss of sensation (peripheral) or very rarely in lepra reaction (both type-1 and type-2 reaction) and are the presenting features of Lucio's phenomenon [1, 2]. Type-2 lepra reaction also known as erythema nodosum leprosum (ENL) characteristically presents as nodules over the face arms and legs. When severe, it can rarely manifest as ulcerative skin lesions (erythema necroticans). We describe one such case of young male who presented with multiple skin ulcers, maculopapular rash, fever, bilateral pulmonary infiltrates and peripheral neuropathy.
Case report
A 40-year-old male farmer presented with fever and progressive increase in breathlessness for 15-20 days. Two months prior the patient noticed nonhealing multiple painless ulcers and rash over the legs, abdomen, and chest. He was treated by local practioners, without relief. One and half months later he started having intermittent fever 103-104°F, with chills and rigors associated with progressive breathlessness and dry cough. There was no history of oliguria, hematuria, cough, expectoration, hemoptysis, seizures, focal neurological deficits, orthoponea and paroxysmal nocturnal dysponea. The patient was not diabetic. He did not have any addictions.
 |
| Figure 1 |
|---|
| Figures 1. Ulcers and papular lesions on the leg |
On examination, patient was febrile, tachypneic, with heart rate of 120 per min and blood pressure of 100/60 mm Hg. Pallor was present. Pedal edema, clubbing, icterus, and lymphadenopathy were not present. The oral cavity was normal. Multiple ulcers 10-15 cm in diameter with a clean base, sharply defined borders and slight marginal erythema were present over the legs, abdomen and chest along with patches of purple red macular papular lesions (Figs. 1 and 2). Examination of chest revealed bilateral scattered crepitations. Pan-systolic murmur (grade II) in left parasternal area was present. There was no hepatosplenomegaly, ascites, focal neurological deficits or thickened nerves. A clinical differential diagnosis of infective endocarditis or systemic necrotizing vasculitis was considered.
 |  |
| Figure 2 | Figure 3 |
|---|---|
| Figures 2 and 3: Ulcers and papular lesions on the trunk | |
Investigations showed hemoglobin 9.0 gm/dl (peripheral blood film showed dimorphic anemia, with a reticulocyte count of 3 %), total leucocyte count 7800/µl with a differential of 75 percent neutrophils, 15 percent lymphocytes, 4 percent monocytes and 5 percent eosinophils, platelets 0.4 million/µl, ESR 65mm in first hour by Westergren method. His biochemical profile revealed elevated liver enzymes with hypoalbuminemia (total serum bilirubin 0.7 mg/ dl, serum alkaline phosphatase 553 mg/ dl, AST/ ALT 110/148 IU/ L, serum proteins/ albumin 6.6/2.8), fasting blood sugar 106 mg/dl, normal serum electrolytes and renal functions. Urine routine examination was unremarkable. Arterial blood gas analysis revealed respiratory alkalosis, (SaO2 94 percent, pH 7.50, PaCO2 24.7, PaO2 84.7, HCO3- 19.3). Mantoux test was non-reactive.
Immunological work up was not contributory (ANCA and ANF were negative by immunofluorescence, serology for HIV, HBsAg, Anti HCV, VDRL and Brucella were all non reactive).
Bilateral pulmonary infiltrates were present on chest X-ray. CT scan of chest showed multiple lung abscesses . Ultrasound of abdomen was normal. Echocardiography revealed vegetations on tricuspid valve with moderate tricuspid regurgitation. Blood cultures and swabs from wounds were sterile. No organism was isolated from bronchoalveolar lavage specimen. Nerve conduction velocities were consistent with polyneuropathy in lower limbs.
 |  |
| Figure 4 | Figure 5 |
|---|---|
| Figure 4. Chest X Ray (PA view) showing bilateral pulmonary infiltrates Figure 5. CT Scan of the chest showing bilateral small abscesses | |
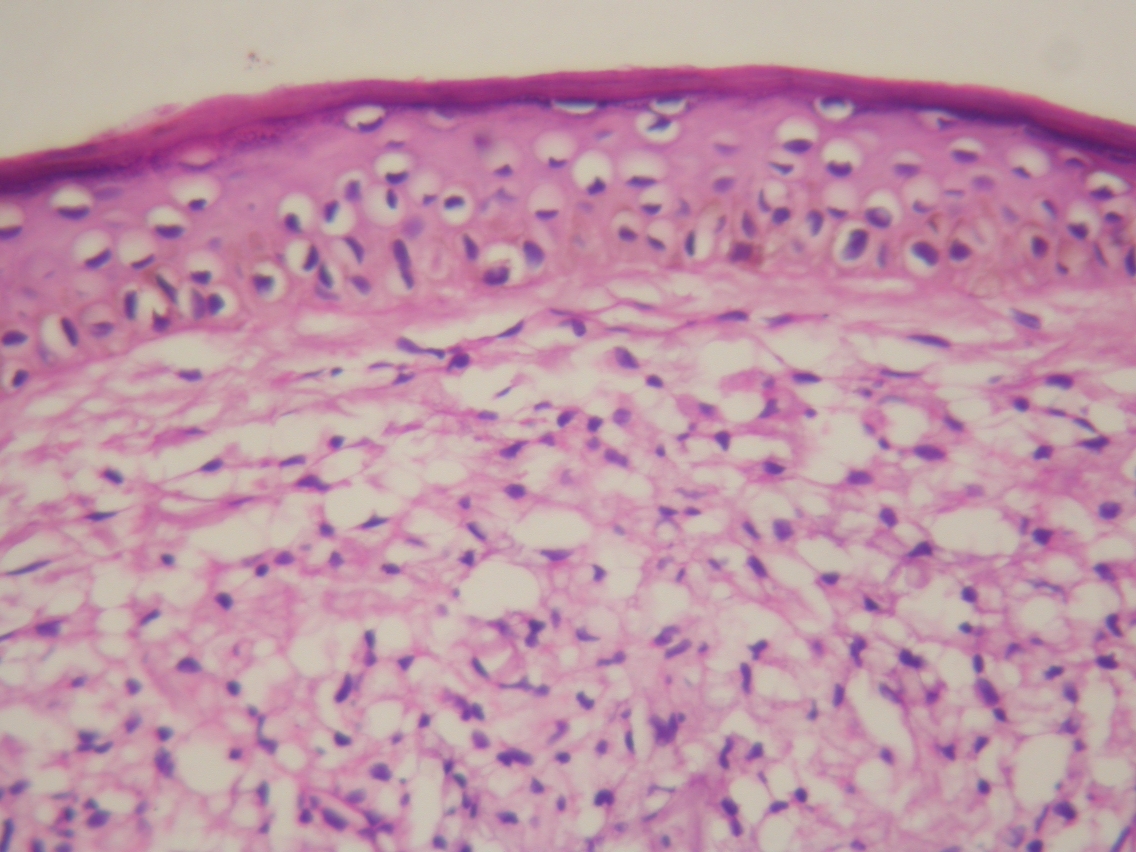
Skin biopsy from margin of ulcer showed thinned out epidermis with diffuse sheets of foamy macrophages centered around adenexal structures. Grenz zone was preserved between the infiltrate and overlying epidermis. AFB stain for lepra bacilli was positive with heavy infiltration of dermis by lepra bacilli. A final diagnosis of ENL with right sided native valve endocarditis with septic embolization to lungs was made.
 |  |
| Figure 6 | Figure 7 |
|---|---|
| Figure 6. Histopathology slide (100X) from margin of ulcer showing thinned out epidermis with diffuse sheets of foamy macrophages
centered around adenexal structures. Grenz zone is well preserved between the infiltrate and overlying epidermis Figure 7. Histopathology slide from ulcer margin (ZN Stain, 1000X) showing heavy infiltration of dermis by lepra bacilli | |
Multi drug therapy for leprosy was started in addition to treatment for infective endocarditis (Cloxacillin 2 gm 6 hourly for 6 weeks with Amikacin 375 mg BD for 2 weeks). Patient became afebrile within a week with normalization of liver enzymes. The lesions healed in 1 week. He was discharged after 6 weeks of parenteral therapy and is on follow up with anti-leprosy treatment being continued.
Discussion
Leprosy is a multi organ infectious disease affecting mainly the skin and the nerves. Skin lesions commonly are macules and plaques, rarely papules or nodules. Lesions vary from being hypopigmented with reduced sensations in tuberculoid leprosy to multiple confluent nodular lesions in lepromatous leprosy [1, 2, 3]. Nerves are damaged in two locations, either peripheral nerve trunks near the fibroosseous tunnels or small dermal nerves in the skin lesions. Leprosy is also associated with type-1 and type-2 reactions [1, 2, 3]. Type-1 reactions occurs in patients with borderline leprosy and never with polar leprosy. This reaction manifests with signs of inflammation within macules, papules and plaques with appearance of new lesions and fever [2]. ENL classically presents as tender erythematous nodules on the face arms and legs. It occurs in lepromatous leprosy with skin infiltration and bacterial index of 4 or more [1].
Ulcers are an unusual presentation of leprosy. These occur as a result of loss of sensation (peripheral), ENL (rarely), or due to Lucio's phenomenon [1, 2, 4]. Besides the classic presentation of erythema nodosum, severe ENL very rarely presents as ulcerative skin lesions (erythema necroticans) [4, 5, 6]. Other unusual manifestations of ENL include neuritis, lymphadenopathy, iritis, orchitis, glomerulonephritis, dactylitis and arthritis [2]. Although ENL may precede the diagnosis of leprosy and initiation of therapy, in up to 90 percent of cases it follows institution of therapy [1]. Investigation reveal anemia, leucocytosis, and elevated liver enzymes [2]. On skin biopsy, panniculitis or vasculitis with sheets or clusters of foamy macrophages and dense inflammation composed of polymorhs and sometimes lymphocytes in dermis are seen [2, 4]. ENL is thought to result from immune complex deposition with elevated levels of tumor necrosis factor α (TNF-α) within the lesions. Thalidomide is the drug of choice for severe ENL in young males [7]. Clofazimine has an anti-inflammatory role in ENL and is helpful in such situations [1, 2]. Other drugs beneficial in ENL are corticosteroids and pentoxyfylline [1].
Multisystem involvement (multiple skin ulcers, maculopapular rash, fever, bilateral pulmonary infiltrates, anemia, with peripheral neuropathy) as seen our case can be easily misdiagnosed as systemic necrotizing vasculitis. A close differential diagnosis was of infective endocarditis with secondary septicemia. Any patient presenting with fever and heart murmur, this possibility should always be entertained. This was confirmed by echocardiography in the index case, and computed tomography showing multiple lung abscesses. Right sided endocarditis could not explain the ulcerated skin lesions in the absence of septal defects. The presence of 4+ lepra bacilli in the skin biopsy confirmed the diagnosis. Lucio's phenomenon was ruled out as it is very rare outside Caribbean areas and histopathology was noncontributory in that there was absence of bacilli in vessel wall and thrombosis of dermal vessels was not seen. Because the patient was not an intravenous drug user and had no other valvular lesions, causes of right sided endocarditis could be hematogeneous spread from the ulcers or spread from the intravenous injections which the patient had received earlier.
We presented this case because erythema necroticans can be easily mistaken for systemic necrotizing vasculitis as in this case and it is important for medical teams to be aware of various manifestations of leprosy including some unusual ones.
References
1. Britton WJ, Lockwood DN. Leprosy. Lancet 2004; 363(9416):1209-19. PubMed.2. Gelber RH. Leprosy (Hansens disease). In: Kasper DL, Braunwald E, Fauci AS, Longo DL, Jamison LJ eds. Harrisons Principles of Internal Medicine16th edn. New York: Mc Graw Hill, 2004; 1: 966-72.
3. Diana N, Lockwood J. Leprosy: In; Warrrel DA, Cox TM, Firth JD, Benz EJ eds. Oxford Textbook of Medicine 4th edn, Oxford. Oxford University Press, 2003: 1; 575-82.
4. Davis SV, Shenoi SD, Balachandran C, Pai SB. A fatal case of erythema nectroticans. Indian J Lepr 2002; 74(2): 145-9. PubMed
5. Dixit VB. Diffuse lepromatosis with recurring ulcerative erythema nodosum leprosum. Indian J Lepr 1992; 64(1); 112-3. PubMed
6. Verma KK, Pandhi KR. Necrotic erythema nodosum: a presenting manifestation of lepramatous leprosy. Int J Lepr 1993; 61(2): 293-4. PubMed
7. Jakeman P, Smith WCS. Thalidomide in leprosy reaction. Lancet 1994; 343(8895): 432-3. PubMed
© 2006 Dermatology Online Journal