Mycobacterium mucogenicum: Report of a skin infection associated with etanercept
Published Web Location
https://doi.org/10.5070/D33nh337n8Main Content
Mycobacterium mucogenicum: Report of a skin infection associated with etanercept
James M Shehan MD, Deba P Sarma MD
Dermatology Online Journal 14 (1): 5
Division of Dermatology, Department of Internal Medicine and Department of Pathology, Creighton University School of MedicineAbstract
Mycobacterium mucogenicum is a recently characterized organism that rarely may cause human infections. This rapidly growing mycobacterium is commonly identified in tap water. Both immunosuppressed and immunocompetent patients may develop infections from Mycobacterium mucogenicum. Some patients have experienced lethal disease, including sepsis. Infections occurring in the skin and soft tissues have been described only after a preceding injury. We present the first case of infection with Mycobacterium mucogenicum occurring in a patient on the TNF-α antagonist etanercept and without any prior soft tissue injury.
Nontuberculous mycobacteria (NTM) infections are becoming increasingly common as new therapeutic agents which induce iatrogenic immunosuppression are developed. Because these infections may involve the skin, dermatologists must understand when to consider the possibility of NTM. The TNF-α antagonists are well-known for their ability to reduce immunity, predisposing to infections such as with Mycobacterium tuberculosis. Likewise these agents increase risk for other types of granulomatous infections, including infections with NTM species. We report a case of skin infection due to Mycobacterium mucogenicum that developed in a patient on etanercept.
Clinical Synopsis
 |  |
| Figure 1 | Figure 2 |
|---|
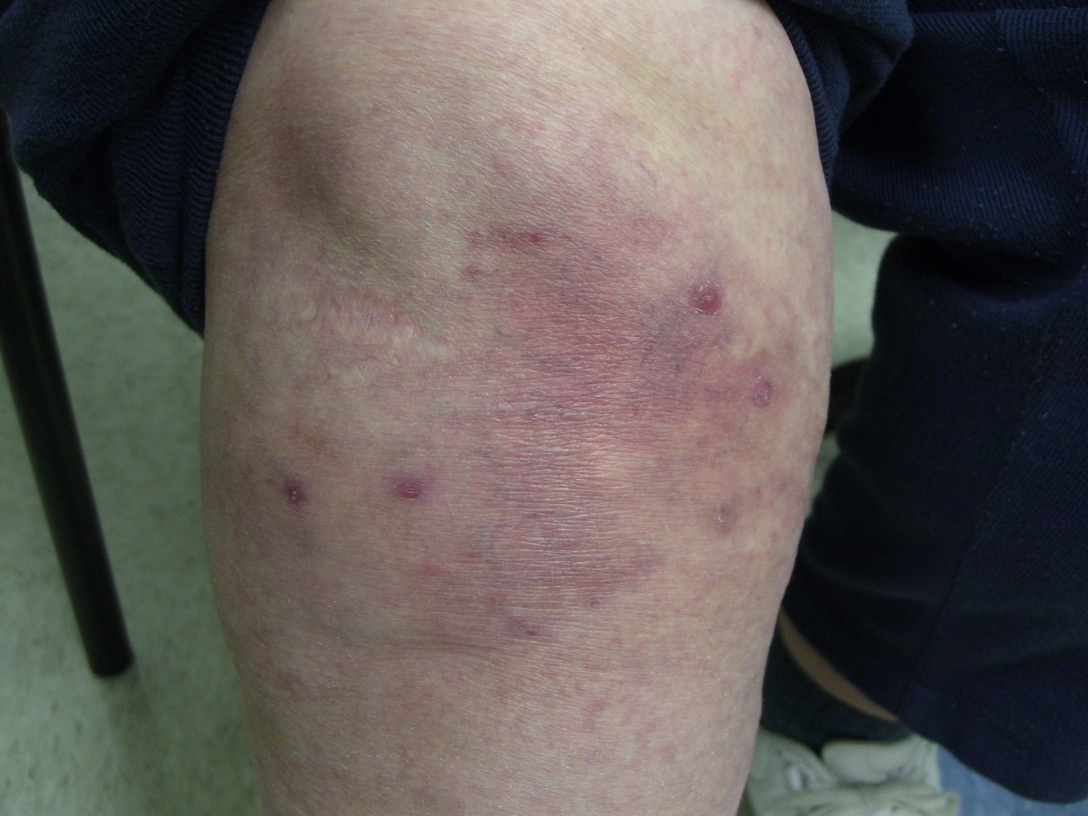
A 61-year-old woman presented with a 3-month history of recurring asymptomatic bumps on her legs. These lesions would periodically ulcerate and drain a cloudy, yellow exudate. The patient suffered from rheumatoid arthritis, managed with low-dose prednisone and etanercept. Constitutionally she felt well. She denied any exposure to whirlpool footbaths, though she did frequently have pedicures in a nail salon. The patient did not recall any previous leg injury. Examination revealed several firm, erythematous papules on her legs, as well as a few deeper dermal to subcutaneous nodules near her ankles (Figs. 1 and 2). A few of the lesions had overlying erosion. No inguinal adenopathy was noted.
 |  |
| Figure 3 | Figure 4 |
|---|---|
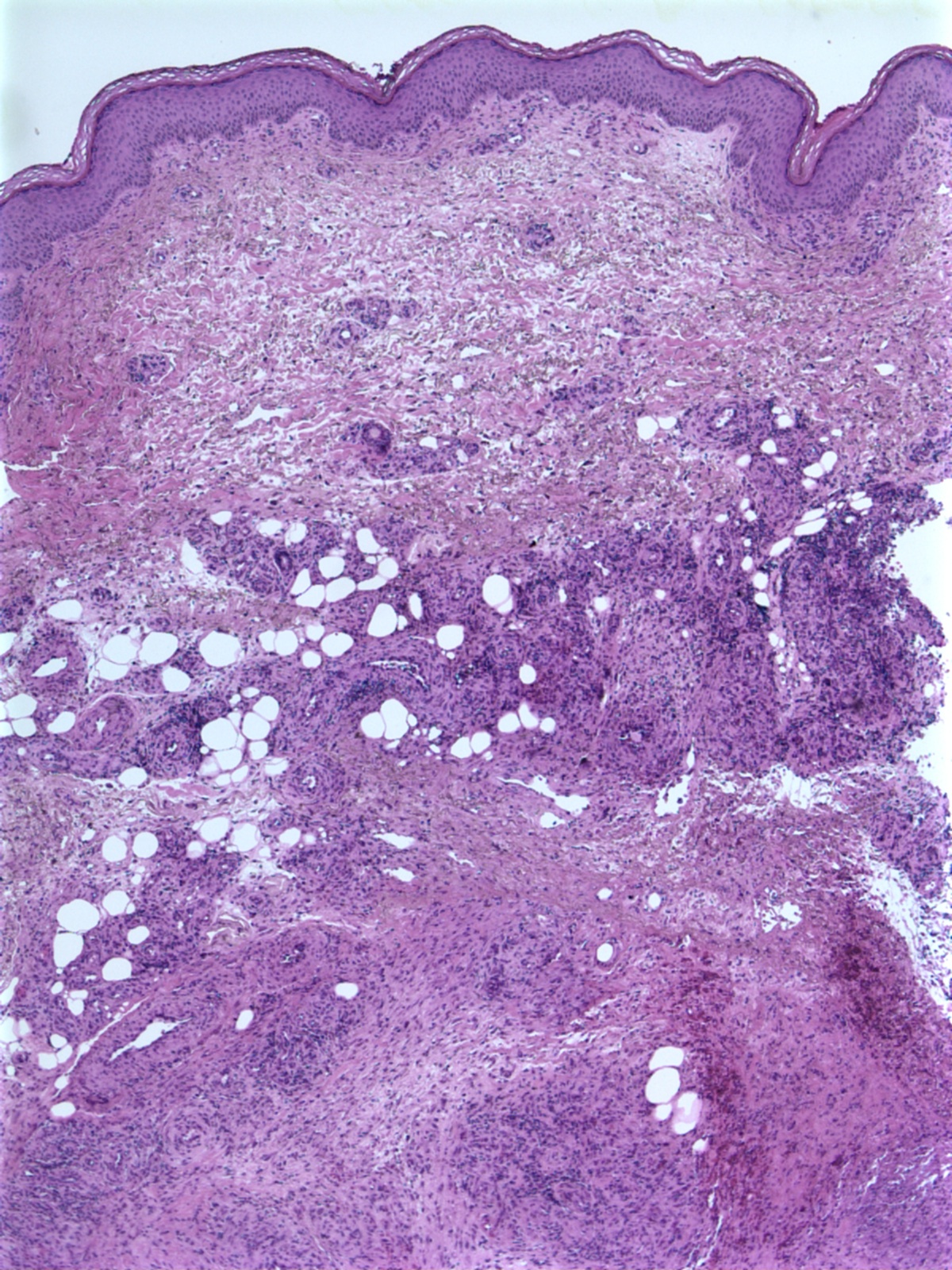
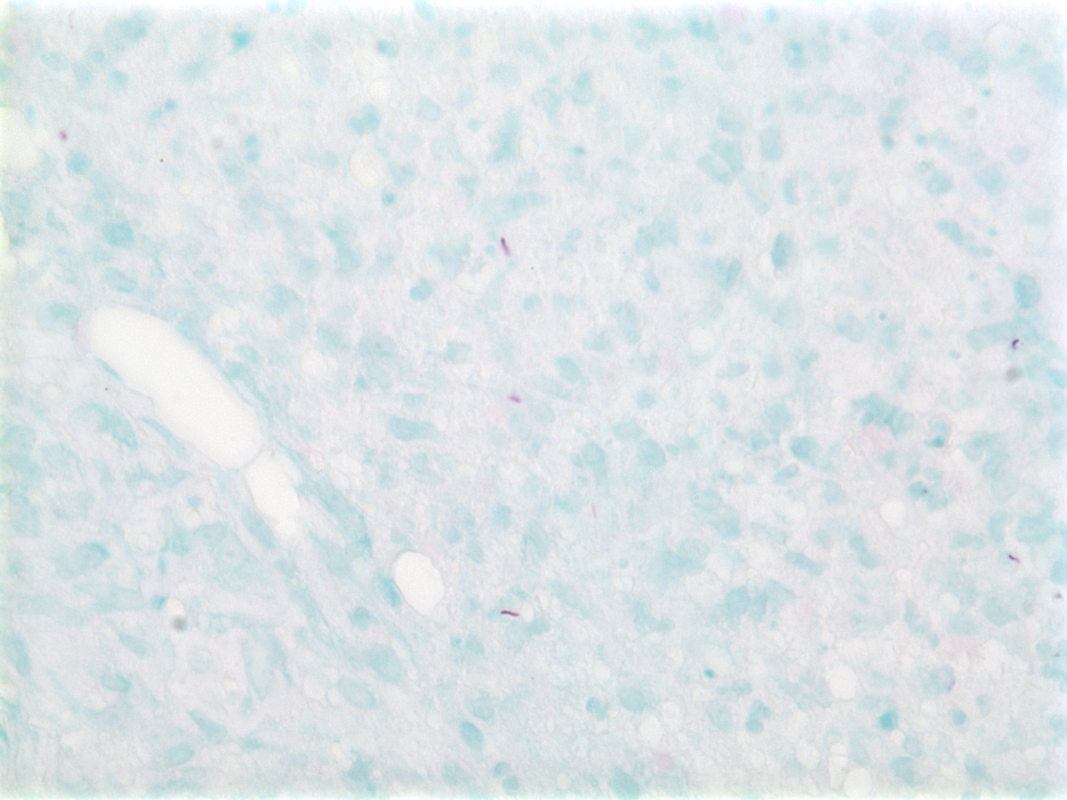
An incisional biopsy was performed from a deep nodule near her ankle. Histologic examination of this lesion showed necrotizing, granulomatous inflammation with mycobacteria identified on an acid fast stain (Figs. 3 and 4). Additionally, a culture grew Mycobacterium mucogenicum.
Her therapy entailed both discontinuing the etanercept and initiating systemic antimicrobials. Based on the identified susceptibilities of the isolates of M. mucogenicum, the patient was started on clarithromycin 500 mg BID and minocycline 100 mg BID. Continuous treatment with these medications is planned for 6 months and further follow-up is pending.
Discussion
TNF-α is a cytokine known to have roles in the resistance to certain infectious organisms and in the etiology of some inflammatory diseases [1, 2]. TNF-α is derived from stimulated mononuclear cells and is critical in early inflammatory pathways, particularly those important for protection from M. tuberculosis [3]. In contrast, TNF-α is also essentially involved in the inflammatory pathways of chronic diseases such as psoriasis, rheumatoid arthritis, and inflammatory bowel disease [2, 3]. The TNF-α antagonists that have been approved by the FDA for inflammatory diseases presently include infliximab, etanercept, and adalimumab [1]. Not surprisingly, this class of medications has been associated with infectious complications—tuberculosis is the most commonly encountered infection [1]. Other NTM infections have been reported in patients on TNF-α antagonists, including a case of M. abscessus infection in the soft tissue of the leg [1]. This particular infection, reported in 2005, was the first case of a rapidly growing mycobacterial infection in the setting of TNF-α antagonist usage yet reported [1]. Of all the TNF-α antagonists, infliximab seems to have the highest risk of associated mycobacterial infections [1, 2, 3]. TNF-α antagonists likely increase the risk for mycobacterial infections through a few different mechanisms. TNF-α functions in granuloma formation and also by stimulating the ability of macrophages to destroy mycobacterial species-with inhibition of these activities by the new biologic agents, infections are able to gain a foothold more readily [1]. In comparison to etanercept, infliximab and adalimumab stimulate apoptosis of monocytes, likely contributing to the increase risk of mycobacterial infections with these two agents [4]. Additionally, infliximab and adalimumab have the added ability to inhibit interferon gamma production and T cell activation [3]. Interferon-γ is very important in immune protection against M. tuberculosis [3].
M. mucogenicum is a recently characterized rapidly growing mycobacterium, formerly known as M. chelonae-like organism [5, 6]. Although first described in 1982 as M. chelonae-like organism, the name M. mucogenicum was not proposed until 1995 by Springer et al. based on 16S rRNA gene sequencing [5, 7, 8]. On culture media, this organism usual exhibits a mucoid appearanceon this basis the species name mucogenicum was recommended in that same report [8]. Additionally, several biochemical characteristics may suggest that a cultured rapidly growing mycobacterium is from the mucogenicum species including the following: positive arylsulfatase reaction, positive citrate on Simmons culture media, nitrate reduction, positive pyrazinamidase, positive urease, positive tween-80 hydrolysis, acid production from mannitol and fructose, and lack of acid production from sorbitol and inositol [7]. Presently, 16S-rRNA gene sequencing is the primary method used to differentiate M. mucogenicum from other rapidly growing mycobacteria species that are cultured in many laboratories [9]. Of note, NTM have been demonstrated to colonize medical devices and drinking water supplies [6, 10]. One study identified that 3 percent of samples from drinking water supply systems from 42 different sources in 21 states contained NTM, with M. mucogenicum isolated most commonly [6]. Apparently, NTM can even live in chlorinated water supplies [10].
M. mucogenicum infections are rare, but have been most commonly reported in patients undergoing peritoneal dialysis, as post-traumatic soft tissue infections, and as catheter-related sepsis [5, 7]. Considering all of this information, some institutions have taken steps to protect central venous catheter and intravenous line sites at times when a patient may have contact with tap water, such as during bathing [10]. Other situations involving infection with M. mucogenicum have included granulomatous hepatitis, pneumonia in an AIDS patient, and central nervous system infections [5, 7, 11]. Immunosuppressed patients, especially those with AIDS or malignancy, seem to be most at risk [7]. One of the largest outbreaks of this infection involved bacteremia in 35 patients after bone marrow transplantation at a hospital in Minnesota [10]. However, some cases have occurred in immunocompetent patients [5]. To our knowledge, the case we present is the first reported infection with M. mucogenicum in the setting of immunosuppression induced by a TNF-α antagonist. It also appears to be the first skin infection with this organism in a patient who did not have a preceding soft tissue injury.
Although various agents may be utilized in the treatment of M. mucogenicum, there is no standard regimen [12]. This is likely because this organism is resistant to several drugs, infections with it are uncommon, and despite aggressive therapy, many of the patients with visceral infections have died [5, 11, 13]. Several drugs have shown in vitro activity against this NTM, including the following: amikacin, ciprofloxacin, clarithromycin, minocycline, and linezolid [5, 7, 12]. In vitro resistance to vancomycin, doxycycline, rifamipin, and isoniazid has been identified [5, 7, 11, 12]. For more severe infections, a combination of two or more agents should be considered [13]. Publications by Adekambi et al (2006) and Fonteyn et al (2005) have excellent tables on antimicrobial susceptibilities for M. mucogenicum that may be consulted when choosing therapeutic agents [5, 7]. Of foremost importance is to have a high index of suspicion for this type of infection, particularly in immunosuppressed patients.
References
1. Mufti AH, Toye BW, McKendry RR, Angel JB. Mycobacterium abscessus infection after use of tumor necrosis factor α inhibitor therapy: case report and review of infectious complications associated with tumor necrosis factor α inhibitor use. Diagn Microbiol Infect Dis. 2005 Nov;53(3):233-8. PubMed2. Wallis RS, Broder MS, Wong JY, Hanson ME, Beenhouwer DO. Granulomatous infectious diseases associated with tumor necrosis factor antagonists. Clin Infect Dis. 2004 May 1; 38(9):1261-5. PubMed
3. Saliu OY, Sofer C, Stein DS, Schwander SK, Wallis RS. Tumor-necrosis-factor blockers: differential effects on mycobacterial immunity. J Infect Dis. 2006 Aug 15;194(4):486-92. PubMed
4. Shen C, Assche GV, Colpaert S, Maerten P, Geboes K, Rutgeerts P, Ceuppens JL. Adalimumab induces apoptosis of human monocytes: a comparative study with infliximab and etanercept. Aliment Pharmacol Ther. 2005 Feb1;21(3):251-8. PubMed
5. Adekambi T, Foucalt C, La Scola B, Drancourt M. Report of two fatal cases of Mycobacterium mucogenicum central nervous system infection in immunocompetent patients. J Clin Microbiol. 2006 Mar;44(3):837-840. PubMed
6. Covert TC, Rodgers MR, Reyes AL, Stelma GN Jr. Occurrence of nontuberculous mycobacteria in environmental samples. Appl Environ Microbiol. 1999 Jun; 65(6):2492-6. PubMed
7. Fonteyn N, Wauters G, Vandercam B, Degraux J, Avesani V, Vincent V, et al. Mycobacterium mucogenicum sepsis in an immunocompetent patient. J Infect. 2006 Sep;53(3):143-6. PubMed
8. Springer B, Bottger EC, Kirschner P, Wallace RJ Jr. Phylogeny of the Mycobacterium chelonae-like organism based on partial sequencing of the 16S rRNA gene and proposal of Mycobacterium mucogenicum sp. nov. Int J Syst Bacteriol. 1995 Apr;45(2):262-7. PubMed
9. Han XY, De I, Jacobson KL. Rapidly growing mycobacteria: clinical and microbiologic studies of 115 cases. Am J Clin Path. 2007 Oct;128(4):612-21. PubMed
10. Kline S, Cameron S, Streifel A, Yakrus MA, Kairis F, Peacock K, Besser J, Cooksey RC. An outbreak of bacteremias associated with Mycobacterium mucogenicum in a hospital water supply. Infect Control Hosp Epidemiol. 2004 Dec; 25(12):1042-9. PubMed
11. Goldblatt MR, Ribes JA. Mycobacterium mucogenicum isolated from a patient with granulomatous hepatitis. Arch Pathol Lab Med. 2002 Jan;126(1):73-5. PubMed
12. Vargas J, Gamboa C, Negrin D, Correa M, Sandoval C, Aguiar A, Prieto M, Rodriguez-Morales AJ, De Waard J, Yakrus M. Disseminated Mycobacterium mucogenicum infection in a patient with idiopathic CD4+ T lymphocytopenia manifesting as fever of unknown origin. Clin Infect Dis. 2005 Sep 1;41(5):759-60. PubMed
13. Paterson DL, Singh N, Gayowski T, Marino I. Mycobacterium mucogenicum bacteremia in a patient with cirrhosis. J of Clin Gastro. 1998 Dec;27(4):346-7. PubMed
© 2008 Dermatology Online Journal