Relapsing polychondritis
Published Web Location
https://doi.org/10.5070/D33kd3r1xdMain Content
Relapsing polychondritis
Arash K Asadi MD
Dermatology Online Journal 9(4): 3
From the Ronald O. Perlman Department of Dermatology, New York University
Abstract
A 57-year-old man presented with a 2-year history of (1) recurrent swelling of the ears that spared his earlobes and (2) migratory arthralgias. A biopsy specimen of the ear showed a perichondrial infiltrate of lymphocytes, plasma cells, and a few neutrophils. There were acellular foci of underlying cartilage. Relapsing polychondritis is characterized by recurrent inflammation and eventual destruction of cartilaginous tissues, primarily affecting the ears, nose, respiratory tract, and eyes. The condition, which is associated with autoimmunity against type II collagen, has a chronic, relapsing-and-remitting course that can be life-threatening. Treatments include a variety of anti-inflammatory and anti-neutrophilic agents, and the prognosis is variable and depends on which organ systems are involved and the response to therapy.
Clinical summary
History.—A 57-year-old man presented with a 2-year history of recurrent inflammation of both ears. Each episode lasts 1-4 weeks and typically affects only one ear. Recurrences occur approximately every 1-6 months, and have increased in frequency in the past year. There is accompanying joint stiffness and pain affecting his wrists. He denies respiratory symptoms. Treatment with ibuprofen, augmented betamethasone dipropionate cream, and several courses of oral antibiotics that include ciprofloxacin, amoxacillin-clavulanate, and cefuroxime have resulted in minor symptomatic improvement. His other medical conditions include gastric reflux disease treated with omeprazole and rabeprazole, hypercholestrolemia treated with pravastatin and simvastatin, and benign prostatic hypertrophy.
Physical examination.—Erythema, edema, warmth, induration, and mild tenderness of the left ear was present and spared the earlobe. Musculoskeletal examination was unremarkable.

|
|
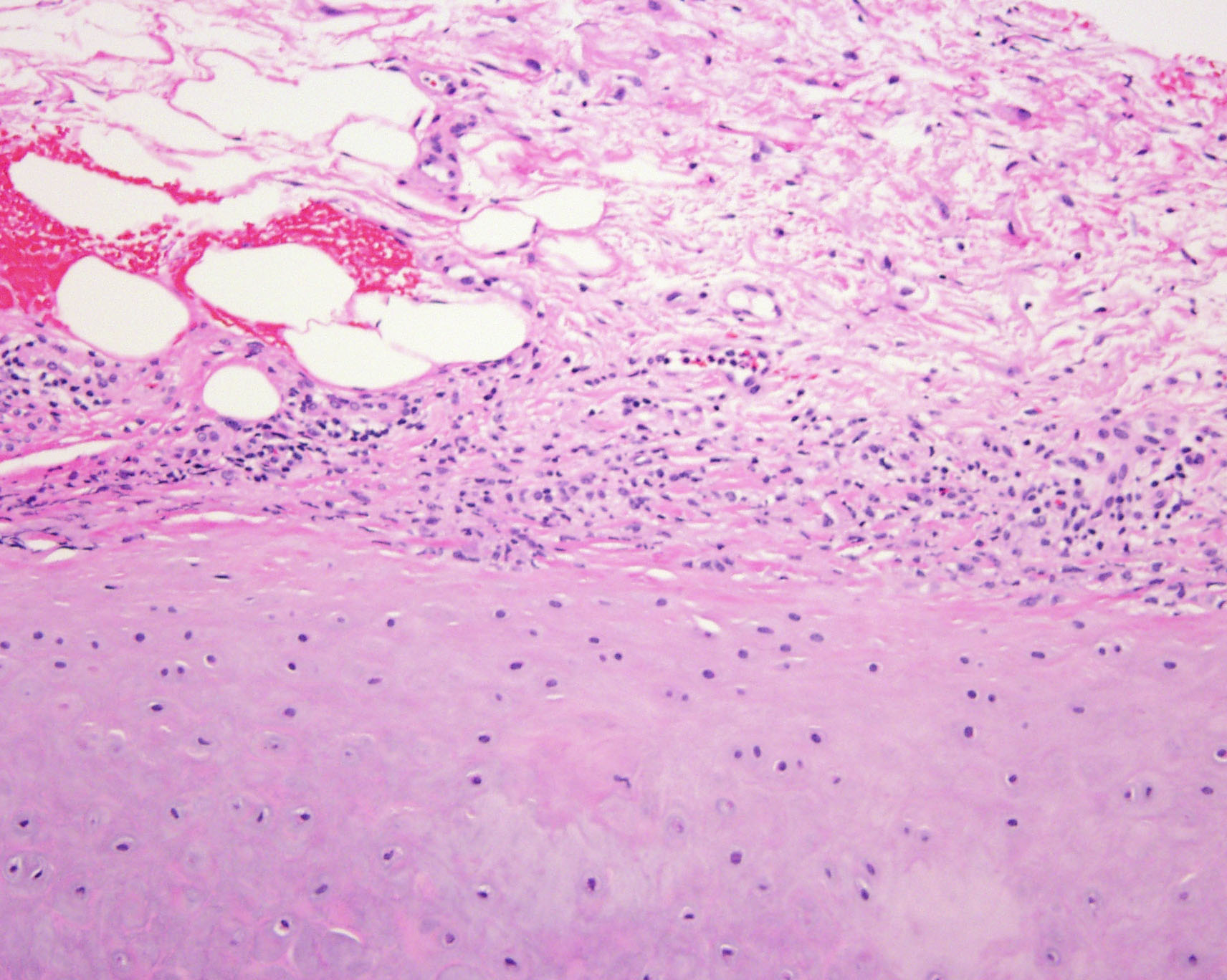
| Figure 4a | Figure 4b |
|---|
Laboratory data.—The erythrocyte sedimentation rate was 17 mm/hr. A complete blood count with differential analysis and uric acid level were normal.
Histopathology.—There is a perichondrial infiltrate of lymphocytes, plasma cells, and a few neutrophils with acellular foci of the underlying cartilage. There is a superficial, perivascular, predominantly lymphocytic infiltrate in the overlying dermis with involvement of the epithelium of the follicular infundibulum.
Diagnosis.—Relapsing polychondritis.
Comment
Relapsing polychondritis is characterized by recurrent inflammation and eventual destruction of cartilage [1, 2]. The disease affects both sexes with equal frequency and is most commonly seen in middle-aged adults. Clinically, there is inflammation of the cartilaginous portion of the ears, which characteristically spares the noncartilaginous earlobes. During each episode only one ear is typically involved. Destruction of auricular cartilage can result in fibrotic changes (cauliflower ear) and occasionally obstructive hearing loss. Inner ear involvement results in nausea, tinnitus, and sensorineural deafness. Involvement of nasal cartilage causes rhinitis with crusting and bleeding and eventual saddle-nose deformity. Hoarseness, coughing, and dyspnea may result from involvement of tracheobronchial cartilage. Bronchial collapse can require stenting or continuous positive pressure respiratory support. Ophthalmologic evaluation may show conjunctivitis, keratitis, episcleritis, or iritis. Migratory mono- and oligo-articular arthritis affecting large and small joints is often present. Leukocytoclastic vasculitis is commonly seen, and aortic involvement with aneurysm formation can require surgical correction.
The diagnostic criteria for relapsing polychrondritis include the presence of at least three of the following: bilateral auricular chondritis, nonerosive seronegative polyarthritis, nasal chondritis, ocular inflammation, respiratory chondritis, and audiovestibular damage [1]. However, the presence of only auricular chondritis with appropriate histologic findings may often be sufficient for diagnosis. The only consistent laboratory finding is an elevated erythrocyte sedimentation rate.
IgG antibodies to type II collagen, which is restricted to and is the predominant collagen of cartilage, can be detected in one-half of patients, with titers corresponding to disease activity [1]. These antibodies can be found circulating in serum or bound to cartilage and can be transferred to a fetus resulting in neonatal chondritis. There is an association with HLA-DR4, and one-third of patients suffer from other autoimmune disorders. In MAGIC syndrome (mouth and genital ulcers with inflammed cartilage), an overlap with Behçet disease is present.
Treatment options include colchicine, indomethacin, and dapsone [1, 2]. In severe or refractory cases, systemic glucocorticoids are indicated, and cyclosporine and methotrexate can serve as steroid-sparing agents. The course of the disease is chronic and recurrent with a variable prognosis. Each episode generally resolves within a few weeks, but recurrences typically occur within weeks to months. Up to one third of patients die from the disease, usually as a result of airway collapse or cardiovascular involvement.
References
1. Trentham DE, Le CH. Relapsing polychrondritis. Ann Intern Med 1998;129:114.2. Cohen PR, Rapini RP. Relapsing polychrondritis. Int J Dermatol 1986;25:280.
© 2003 Dermatology Online Journal