A child with giant cell tumor of tendon sheath
Published Web Location
https://doi.org/10.5070/D33076n54xMain Content
A child with giant cell tumor of tendon sheath
Takashi Ueno MD PhD, Shin-ichi Ansai MD PhD, Tokuya Omi MD PhD, Seiji Kawana MD PhD
Dermatology Online Journal 17 (5): 9
Department of Dermatology, Musashi-Kosugi Hospital, Nippon Medical School, JapanAbstract
A giant cell tumor of tendon sheath (GCTTS) is a soft tissue tumor consisting principally of a proliferation of synovial cells arising from a tendon sheath. GCTTS is the second most common tumor of the hand in general and a majority of GCTTS cases are in patients between 20 and 50 years of age, whereas pediatric cases of GCTTS are uncommon. This report presents the case of a nine-year-old girl with GCTTS arising on her right index finger.
Introduction
A giant cell tumor of tendon sheath (GCTTS) is a gradually-developing, painless soft tissue tumor that contains a circumscribed proliferation of synovial cells accompanied by multinucleate giant cells, foam cells, siderophages, and inflammatory cells [1, 2]. GCTTS is a common tumor in general, although GCTTS uncommonly occurs in children [3]. This report describes a case of GCTTS arising from the flexor tendon sheath of the index finger in a nine-year-old girl.
Case report
A nine-year-old girl presented with a 6 month history of a painless nodule on her right index finger. The patient and her parents had no memory of any injury to the digit.
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. A dome-shaped nodule with normal skin color on the surface, located on the volar-radial aspect of the proximal phalangeal
part of the right index finger Figure 2. X-ray showing a soft tissue mass without calcification and no evidence of erosion of the phalanx. | |
A clinical examination revealed a 13 mm x 13 mm dome-shaped nodule with normal skin color on the surface, located on the volar-radial aspect of the proximal phalangeal part of the right index finger (Figure 1). The nodule was well-confined, smooth, elastic, firm, and not adherent to the overlying skin, but held in place by the basement structures. There was no translucency through the tumor and the patient experienced no tenderness or radiating pain during the examination. There was normal sensory perception in the digit and range of motion was normal in the related joints. An X-ray photograph showed a soft tissue mass without calcification and no evidence of erosion of the phalanx (Figure 2).
 |  |
| Figure 3 | Figure 4 |
|---|---|
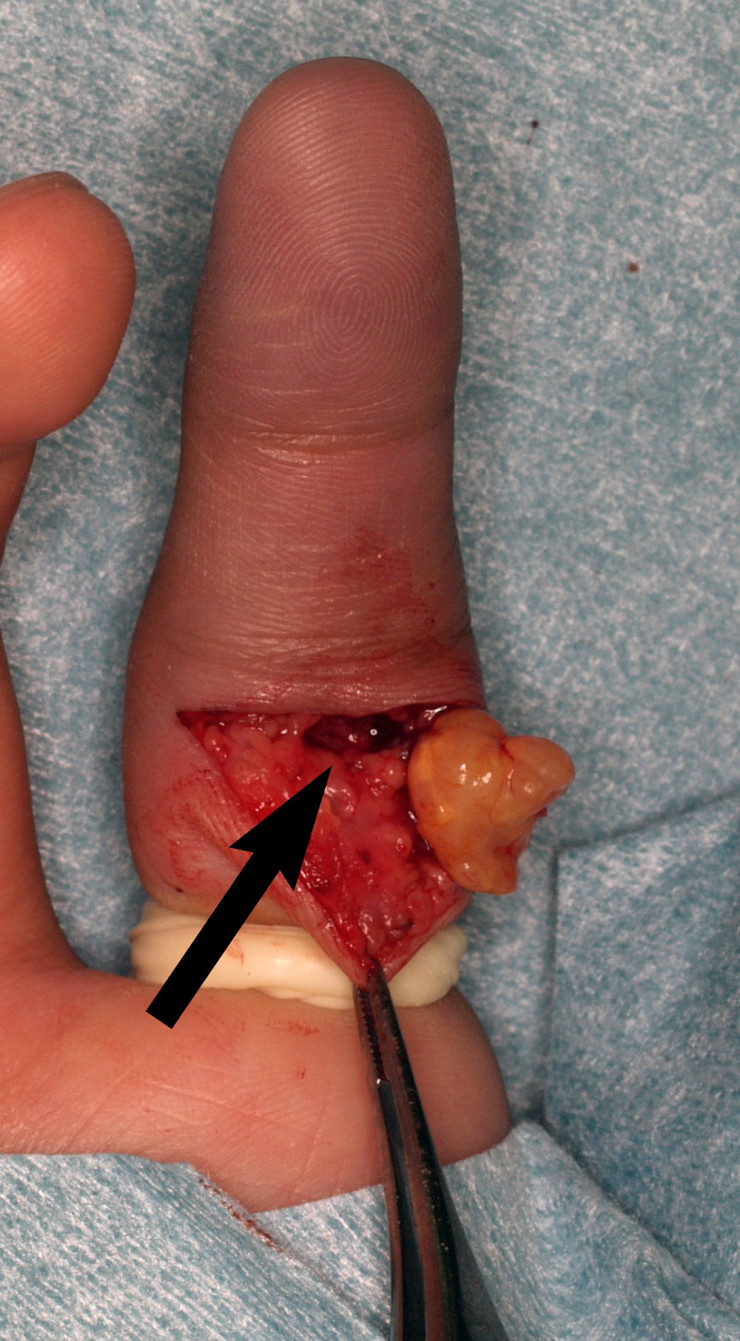
| Figure 3. A well-demarcated yellowish lobulated tumor with a thin fibrous capsule is seen. The tendon sheath to which the
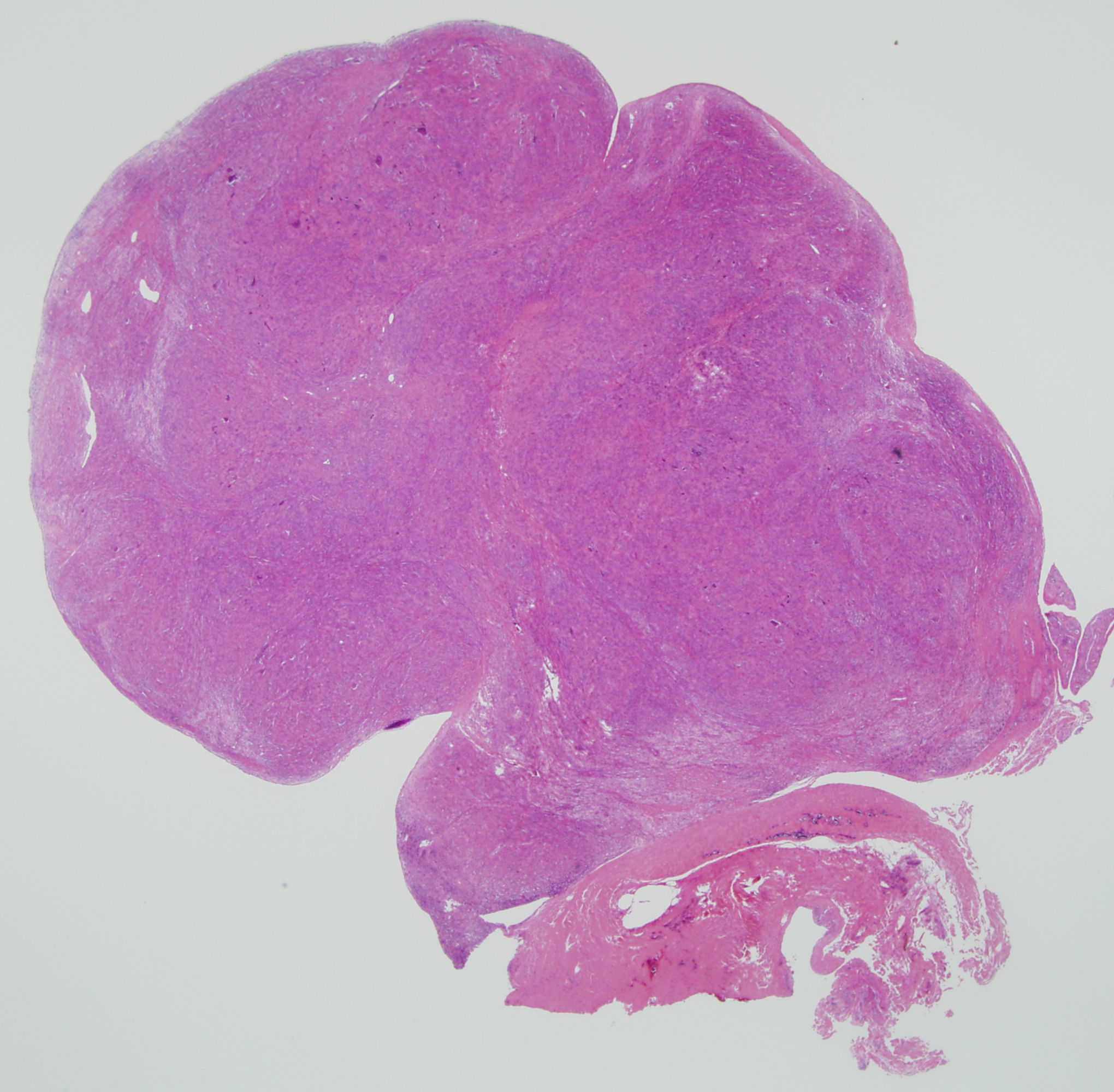
tumor adhered was also resected (arrow). Figure 4. Low magnification of an H&E stained specimen revealed a circumscribed lobulated nodule. | |
 |
| Figure 5 |
|---|
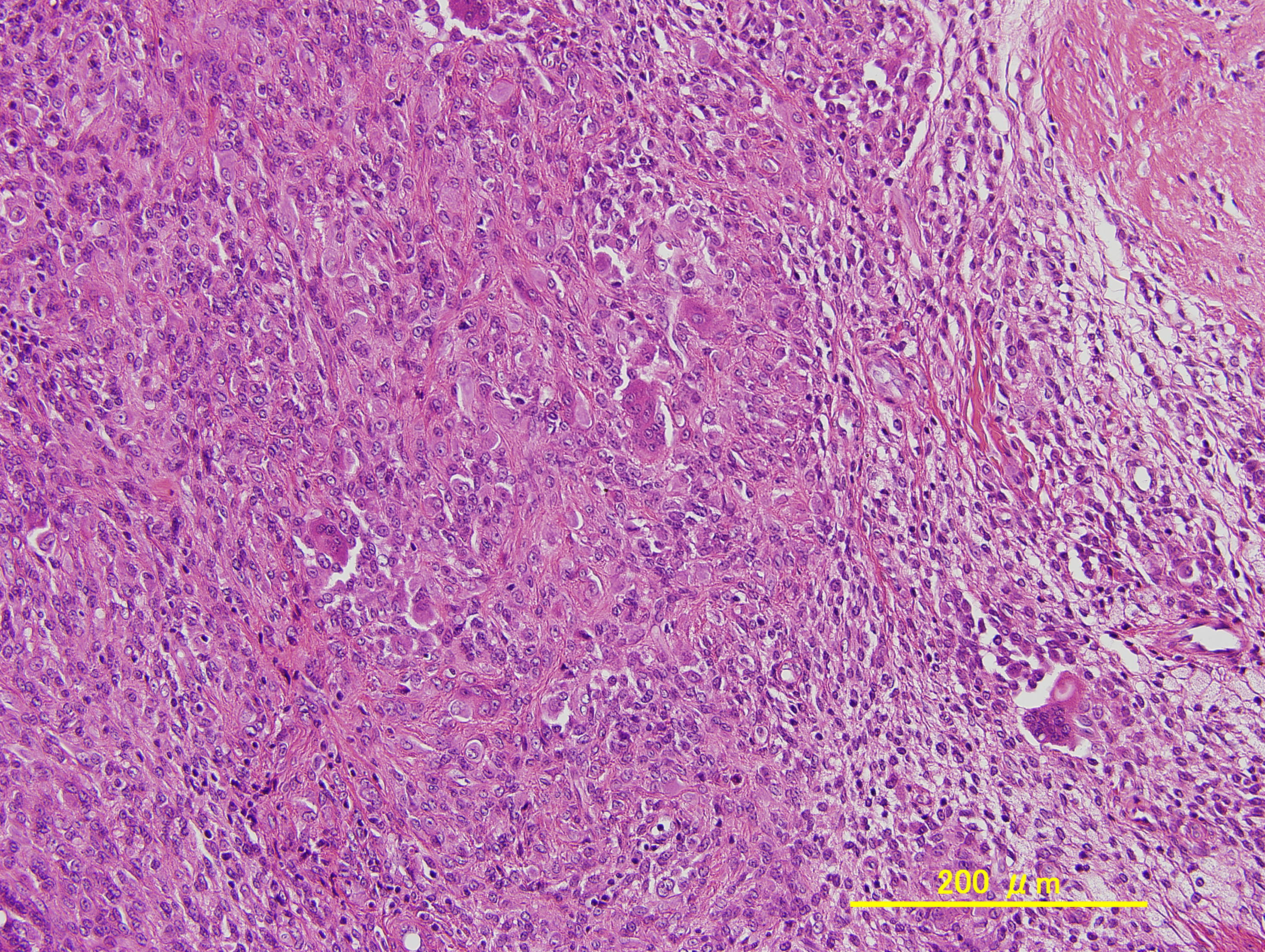
| Figure 5. Histiocytes with abundant eosinophilic cytoplasm, fibroblasts, collagen hyperplasia, multinucleate giant cells and foam cells were observed (H&E, x200) |
A complete resection was performed under local anesthesia (Figure 3). A well- demarcated yellowish lobulated tumor with a thin fibrous capsule arose from the flexor tendon sheath. The tendon sheath that adhered to the tumor was also resected. The histological examination revealed a circumscribed lobulated nodule (Figure 4). The tumor contained histiocytes with abundant eosinophilic cytoplasm, fibroblasts with fusiform-shaped nuclei, collagen hyperplasia, multinucleated giant cells, and foam cells (Figure 5). Increased cellularity and nuclear mitoses were rarely seen. The findings were consistent to with those of a GCTTS. No recurrence has been observed after 18 months.
Discussion
GCTTS is synonymous with a tenosynovial giant cell tumor, localized type, or nodular tenosynovitis [1]. GCTTS was first reported in 1852 by Chassaignac who described a nodule arising in a flexor tendon sheath of the finger as a cancer of the tendon sheath [2]. Jaffe et al [4] characterized the synovium of the tendon sheath, bursa, and synovial membrane of the joint as an anatomic unit that could present a common family of lesions. The lesions were classified as GCTTS (or nodular tenosynovitis) and circumscribed or diffuse forms of pigmented villonodular synovitis (PVS).
GCTTS commonly occurs in the patients between 20 and 50 years of age and uncommonly in children under 10 years old [2, 3, 5, 6]. Myers and Masi [7] surveyed 166 new cases with GCTTS (N=117) or PVS (N=49) in 1980 and reviewed the previously reported literature, including a total of 1301 lesions; 69 percent were GCTTS, 8 percent were circumscribed PVC, and 23 percent were diffuse PVC. No patient less than 10 years old was reported to have GCT or PVS. The authors also found only nine such children in the literature. Subsequent studies [5, 8, 9, 10] have revealed that the incidence of GCTTS patients less than 10 years old is 0 to 4.3 percent. There have been no studies investigating why GCTTS is rare in childhood.
Generally, hand tumors are rare in children [11]. Three studies have reviewed pediatric hand tumors. Woods et al [12] analyzed 44 pediatric patients with hand tumors and reported that hemangioma (30%) was the most common, followed by juvenile dermatofibroma (14%), ganglion cyst (7%); no patients were diagnosed with GCTTS. They suggested that the result might not represent the normal distribution because the study included mainly patients hospitalized for specific therapy. Azouz et al [13] studied 23 children with soft tissue tumors of the hand and wrist and found that 39 percent had blood or lymph vessel tumor, 17 percent GCTTS, 17 percent tumoral calcinosis, and 12 percent soft tissue chondroma. Colon and Upton [11] reviewed 349 cases of pediatric hand tumors and revealed that a retained foreign body (21%) was the most common, followed by ganglion cyst (16%), vascular malformations (14%), and retinacular cyst (9%). They also reported nodular tenosynovitis developing in 3 percent of their patients. Therefore, GCTTS may be uncommon in children with hand tumors, even though GCTTS is the second most common tumor of the hand following ganglion cyst in general [2, 14].
GCTTS recurs locally in 4-30 percent of cases [1]. Recurrence seems to develop in patients that had lesions with high cellularity and mitotic activity or those with incomplete excision with residual tumor left beneath the deep margin [1, 2, 14]. Al-Qattan [14] classified 43 cases of GCTTS into two types, based on whether the entire tumor was surrounded by a pseudocapsule (type I), or not (type II). The author reported that 30 cases of type I did not recur whereas 5 of 13 cases of type II did. Gholve et al [3] retrospectively reviewed 29 cases of GCTTS in patients younger than 18 years old. They found no recurrence in patients that were followed and hypothesized that GCTTS in children was less likely to recur than those in adults.
The current case had some unusual features. It was a well-demarcated nodule with a fibrous capsule, representing Al-Qattan’s type I and it was excised completely including a portion of the tendon sheath from which the tumor arose. Little of the tumor showed high cellularity or mitotic activity and the patient was a child. Those factors are often characteristic of nonrecurring GCTTS. Therefore recurrence is not expected in this patient.
References
1. Somerhausen NS, Dal Cin P. Giant cell tumour of tendon sheath. In: Fletcher CD, Krishnan Unni K, Mertens F, eds. Pathology And Genetics of Tumours of the Soft Tissues And Bones (World Health Organization Classification of Tumours). Lyon: IARCPress, 2002; 110-111.2. Weiss SW, Goldblum JR. Benign tumors and tumor-like lesions of synovial tissue. In: Weiss SW, Goldblum JR ed: Enzinger and Weiss’s Soft Tissue Tumors, 5th: St. Louis: Mosby, 2007; 769-88.
3. Gholve PA, Hosalkar HS, Kreiger PA, Dormans JP. Giant cell tumor of tendon sheath: largest single series in children. J Pediatr Orthop 2007 Jan-Feb; 27(1):67-74. [PubMed]
4. Jaffe HL, Lichtenstein L, Sutro CJ. Pigmented villonodular synovitis, bursitis and tenosynovitis. Arch Pathol 1941; 31: 731-765.
5. Biddulph SL. Synovial lesions. In: Bogumill GP, Fleegler EJ eds. Tumors of the Hand and Upper Limb. Churchill Livingstone 1993; 183-191.
6. Hulse N, Watson SJ. Giant cell tumour of tendon sheath in a child: a case report. Hand Surg 2005 Jul; 10(1):97-100. [PubMed]
7. Myers BW, Masi AT. Pigmented villonodular synovitis and tenosynovitis: a clinical epidemiologic study of 166 cases and literature review. Medicine (Baltimore) 1980 May; 59(3):223-38. [PubMed]
8. Rao AS, Vigorita VJ. Pigmented villonodular synovitis (giant-cell tumor of the tendon sheath and synovial membrane). A review of eighty-one cases. J Bone Joint Surg Am 1984 Jan; 66(1):76-94. [PubMed]
9. Ushijima M, Hashimoto H, Tsuneyoshi M, Enjoji M. Giant cell tumor of the tendon sheath (nodular tenosynovitis). A study of 207 cases to compare the large joint group with the common digit group. Cancer 1986 Feb 15; 57(4):875-84. [PubMed]
10. Darwish FM, Haddad WH. Giant cell tumour of tendon sheath: experience with 52 cases. Singapore Med J. 2008 Nov; 49(11):879-82. [PubMed]
11. Colon F, Upton J. Pediatric hand tumors. A review of 349 cases. Hand Clin 1995 May; 11(2):223-43. [PubMed]
12. Woods JE, Murray JE, Vawter GF. Hand tumors in children. Plast Reconstr Surg 1970 Aug; 46(2):130-9. [PubMed]
13. Azouz EM, Kozlowski K, Masel J. Soft-tissue tumors of the hand and wrist of children. Can Assoc Radiol J 1989 Oct; 40(5):251-5. [PubMed]
14. Al-Qattan MM. Giant cell tumours of tendon sheath: classification and recurrence rate. J Hand Surg Br 2001 Feb; 26(1):72-5. [PubMed]
© 2011 Dermatology Online Journal