Transient peripheral facial nerve paralysis after local anesthetic procedure
Published Web Location
https://doi.org/10.5070/D32zx744fcMain Content
Letter: Transient peripheral facial nerve paralysis after local anesthetic procedure
Aristóteles Rosmaninho1, Inês Lobo1, Mónica Caetano1, Ricardo Taipa2, Marina Magalhães2, Virgílio Costa1, Manuela Selores1
Dermatology Online Journal 18 (4): 15
1. Department of Dermatology, Centro Hospitalar do Porto, Porto, Portugal2. Department of Neurology, Centro Hospitalar do Porto, Porto, Portugal
Abstract
Complications may arise after laser therapy of the face. The most common ones are bleeding and infections; facial nerve paresis or paralysis is rarely reported. We describe a case of a transient peripheral facial nerve paralysis after laser therapy of an epidermal verrucous nevus localized at the left preauricular area.
Introduction
 |
| Figure 1 |
|---|
| Figure 1. Laser therapy of the facial lesion |
Complications such as bleeding and infection as well as neurological adverse effects of the local anesthetics (hypostesia, paresthesia, and anesthesia) related to the damage of sensory nerves may occur after laser therapy of the face [1]. This article describes a case of a transient peripheral facial nerve paralysis after CO2 laser therapy, which has been rarely reported after dermatological procedures and constitutes a rare side effect of local anesthetics.
Case report
A 40-year-old healthy man was treated with laser therapy (CO2 laser) to an epidermal verrucous nevus of 4.5 cm, localized at the left preauricular area.
To obtain anesthesia, 10 mL of 2 percent lidocaine with epinephrine (1:200,000) was administered into the upper subcutaneous tissue using a 30-gauge local anesthetic needle. CO2 laser (CW mode, 5w/cm²) was then performed with no complications.
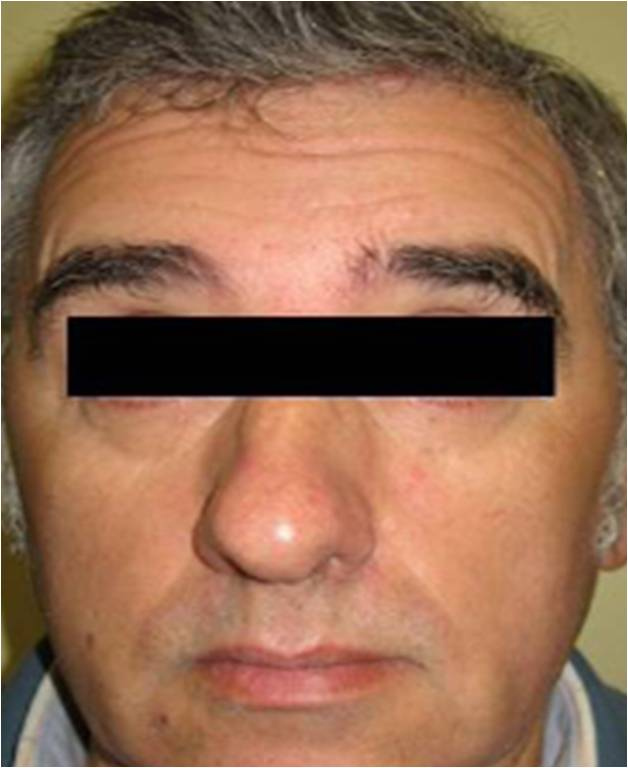
However, in the immediate postoperative course, inability to close the left eyelid was noticed by the patient. The left hemifacial creases and nasolabial fold disappeared. In addition, the forehead unfurrowed and the left corner of the mouth drooped.
 |  |
| Figure 2 | Figure 3 |
|---|---|
| Figure 2. Inability to furrow the left forehead Figure 3. Inability to close the left eye | |
 |  |
| Figure 4 | Figure 5 |
|---|---|
| Figure 4. Paralysis of the left upper lip elevator muscles Figure 5. Resolution of the paralysis | |
The facial sensation was preserved and no other neurologic deficits were observed. He was referred to the Neurology Department and the diagnosis of an incomplete peripheral facial nerve paralysis was made.
The patient fully recovered within 12 hours without any residual weakness of the involved facial muscles (Figure 5).
Discussion
Peripheral facial nerve paralysis as a complication of maxillofacial surgery or dental procedures is not unusual, but this complication has rarely been reported with anesthesia [2, 3].
There have been sporadic reports of facial branch paralysis after surgery, but the involvement of the total facial nerve, as in the present report, is a rare event [4].
The branches of the facial nerve at great risk of injury are the temporal and the marginal mandibular nerves [5]. The temporal branch is prone to injury during surgery on the temple, where it lies superficially. The marginal mandibular branch can be injured at the angle of the mandible.
The facial nerve exits from the cranial base through the stylomastoid foramen, which lies lateral to the styloid process and medial to the mastoid tip. It then travels between the didastric and stylohyoid muscles and enters into the parotid gland. The mean minimal distance of the facial nerve trunk from the skin surface is 22.4 mm, but in a more superficial position distances of 15.7 mm may be found [7]. The main bifurcation is located inside the parotid gland in 85 percent of cases [7]; in the remaining 15 percent it bifurcates proximal to its penetration into the parotid [5].
A central nervous system lesion may be easily excluded because of the isolated facial muscle weakness pattern. Usually the central lesions affecting the facial nerve do not paralyze the forehead. Some motor neurons to the forehead cross sides at the level of the brainstem, so the fibers in the facial nerve going to the forehead come from both cerebral hemispheres [6].
The total nerve involvement leads to the conclusion that the possible injury in this paralysis may have occurred in the main trunk of the facial nerve, before the bifurcation into its main branches (temporal, zygomatic, buccal, marginal mandibular, and cervical). Alternatively, it may have resulted as a consequence of a more superficial and long trunk, with more distal bifurcation in the main branches.
Several mechanisms have been proposed to explain peripheral facial nerve paralysis, including: direct trauma to the nerve from a needle, intraneural hematoma formation, and local anesthetic toxicity [2].
Direct anesthesia of the nerve alone seems to be unlikely because patients usually feel the electric shock sensation at the time of injection of the needle. However, the needle may have reached the blood vessels of the epineurium causing hemorrhage within the nerve that ultimately caused compression. Moreover, most local anesthetics such as bupivacaine, procaine, and lidocaine have a neurotoxic effect. However, this neurotoxitcity usually occurs when the anesthesia is administrated intrathecally [2, 3]. Vasconcelos BC et al, also proposed that postoperative edema in the region of the parotid gland or an alteration in the anesthetic solution could contribute to a temporary facial nerve paralysis after impacted lower third molar surgery [2].
This case should increase clinical awareness of this potential complication. Physicians must be familiar with the facial nerve anatomy when such procedures are executed.
References
1. Koay J, Orengo I. Application of local anesthetics in dermatologic surgery. Dermatol Surg 2002;28:143-8. [PubMed]2. Vasconcelos BC, Bessa-Nogueira RV, Maurette PE, Carneiro SCSA. Facial nerve paralysis after impacted lower third molar surgery: A literature review and case report. Med Oral Patol Oral Cir Bucal 2006;11:E175-8. [PubMed]
3. Tazi M, Soichot P, Perrin D. Facial palsy following dental extraction: report of 2 cases. J Oral Maxillofac Surg 2003;61:840-4. [PubMed]
4. Hendi A. Transient buccal nerve paresis. Dermatol Surg 2008;34:258-60. [PubMed]
5. Salasche S, Bernstein G, Senkarik M. Surgical anatomy of the skin. Notwalk (CT): Appleton & Lange; 1988. Pp. 8-10.
6. Tiemstra JD, Khatkhate N. Bell's palsy: diagnosis and management. Am Fam Physician 2007;76:997-1003. [PubMed]
7. Salame K, Ouknine GER, Arensurg B, Rochkind S. Microsurgical anatomy of the facial nerve trunk. Clin Anat 2002;15:93-9. [PubMed]
© 2012 Dermatology Online Journal