Radiofrequency ablation: A safe and economical modality in treatment of Brooke-Spiegler syndrome
Published Web Location
https://doi.org/10.5070/D32tf564dmMain Content
Radiofrequency ablation: A safe and economical modality in treatment of Brooke-Spiegler syndrome
Savita Chaudhary1 MD Fellow ISD, Surabhi Dayal2 MD
Dermatology Online Journal 18 (8): 7
1. Era's Lucknow Medical College and Hospital Lucknow, Uttar Pradesh, India2. Pt B D Sharma PGIMS, Rohtak, Haryana, India
Abstract
Brooke-Spiegler syndrome is an uncommon disease. Patients have a predisposition to develop cutaneous adnexal neoplasms such as cylindromas, trichoepitheliomas, spiradenomas, trichoblastomas, basal cell carcinomas, follicular cysts, and organoid nevi. Malignant transformation of preexisting tumors also occurs in these individuals. Various techniques have been used for the treatment of trichoepitheliomas and cylindromas including excision, electrocautery, carbon dioxide laser ablation, cryosurgery, and radiotherapy. In our case, cylindromas were ablated by radiofrequency in multiple sittings. Trichoepitheliomas were ablated using coagulation mode with power # 3 to 3.5. Cosmetically acceptable results were obtained in 100 percent of the cylindromas and 70 percent of the trichoepitheliomas (Visual Analog Scale). The radiofrequency ablation technique under different modes can be used in both large tumors as well as smaller ones, especially in developing countries because it is very cost effective and easily accessible.
Disease description and etiopathogenesis
Brooke-Spiegler syndrome (BSS) (OMIM 605041), also known as familial cylindromatosis (OMIM 132700), is an autosomal dominantly inherited tumor predisposition disorder that was reported for the first time in 1842 by Ancell [1]. Cylindromas are slow-growing tumors that are thought to arise from a pluripotent stem cell in the hair follicle. The tumors can vary in size from 0.5 to 6 cm in diameter and are often found in the scalp. They coalesce and form confluent masses, historically termed “turban tumors” [2]. A female preponderance is noted and the clinical phenotype usually manifests by the third decade [3]. Cylindromas typically have a firm consistency and a pink surface with arborizing blood vessels and a yellowish, homogenous macroscopic appearance when bisected. Inherited cylindromas are not exclusively found in familial cylindromatosis; patients with multiple familial trichoepitheliomas (MFT; OMIM 601606) also [4] develop them. An overlap syndrome of these two conditions, Brooke-Spiegler Syndrome (BSS; OMIM 605041), describes patients who develop a heterogeneous group of hair follicle-related tumors, including cylindromas, trichoepitheliomas, and eccrine spiradenomas. The clinical spectrum and tumor heterogeneity support a pluripotent stem cell in the hair follicle as the likely site of tumor induction [5]. Recently, all three conditions have been unified at a genetic level by mutations in the tumor suppressor gene CYLD [6]. The heterogeneous tumors found in BSS warrant specific techniques of removal. Cylindromas are so named because the histological appearance in cross section resembles stacked cylinders. The tumor is based in the dermis and is not encapsulated and surgical planes of cleavage are often not distinct [7]. Conversely, eccrine spiradenomas are often encapsulated and can be removed through small incisions, using techniques typically applied to lipomas. Clinically, they can be distinguished because they are often painful and may have a bluish appearance. Trichoepitheliomas, which are typically less than 5 mm in diameter and found predominantly at the nasolabial folds, may extend into the subcutis.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Pretreatment front view of the face showing trichoepitheliomas Figure 2. Pretreatment left lateral view of face and scalp showing cylindromas | |
 |
| Figure 3 |
|---|
| Figure 3. Pretreatment right lateral view of face and scalp showing cylindromas |
A 46-year-old male presented with a history of multiple flesh colored, pedunclated papules and nodules over the scalp and skin colored papules over face for the 40 years; these were progressively increasing in size and number. Family history was positive in the patient’s maternal grandmother and mother of the maternal grandmother. Clinically, the lesions appeared as multiple flesh colored pedunclated nodules varying from 1 x 1 cm to 3 x 4 cm in size, present over the scalp (including right and left temporal and bilateral pre-auricular regions) (Figures 1, 2, and 3). On palpation they were soft, smooth, non-tender and non-compressible. There were also multiple skin colored papules present in a clustered pattern over the face, including forehead, bilateral cheeks, nose, nasolabial folds, and chin.
Histopathology and diagnosis
 |  |
| Figure 4 | Figure 5 |
|---|---|
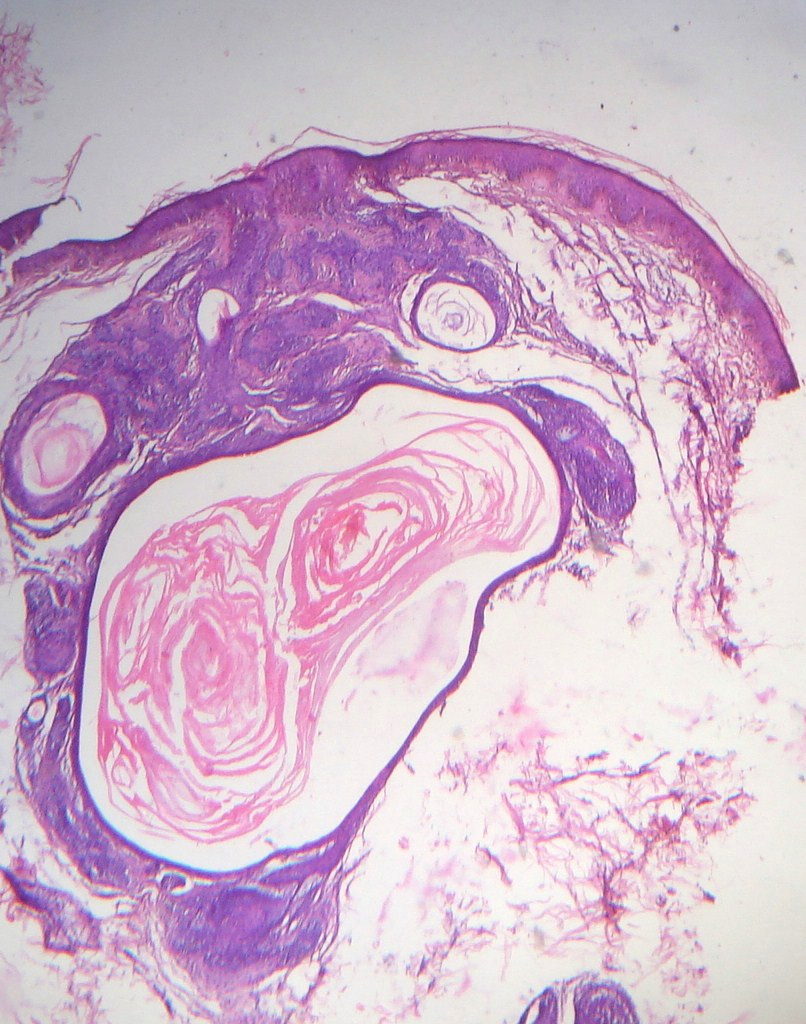
| Figure 4. Photomicrograph of trichoepithelioma showing an unremarkable epidermis and a dermis containing islands of basaloid
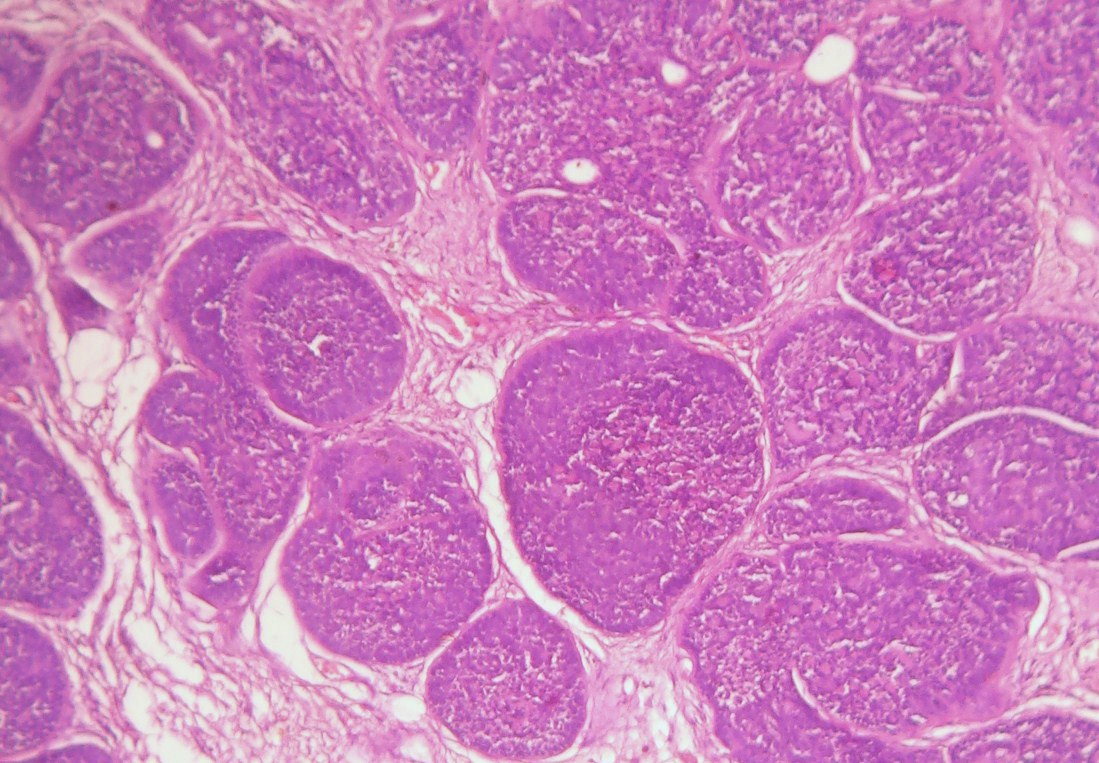
epithelial cells along with horn cysts of varying sizes surrounded by a fibrous stroma (H&E x100) Figure 5. Photomicrograph of cylindroma showing large lobulated nests of basaloid cells arranged in a jig-saw pattern (H&E x100) | |
 |
| Figure 6 |
|---|
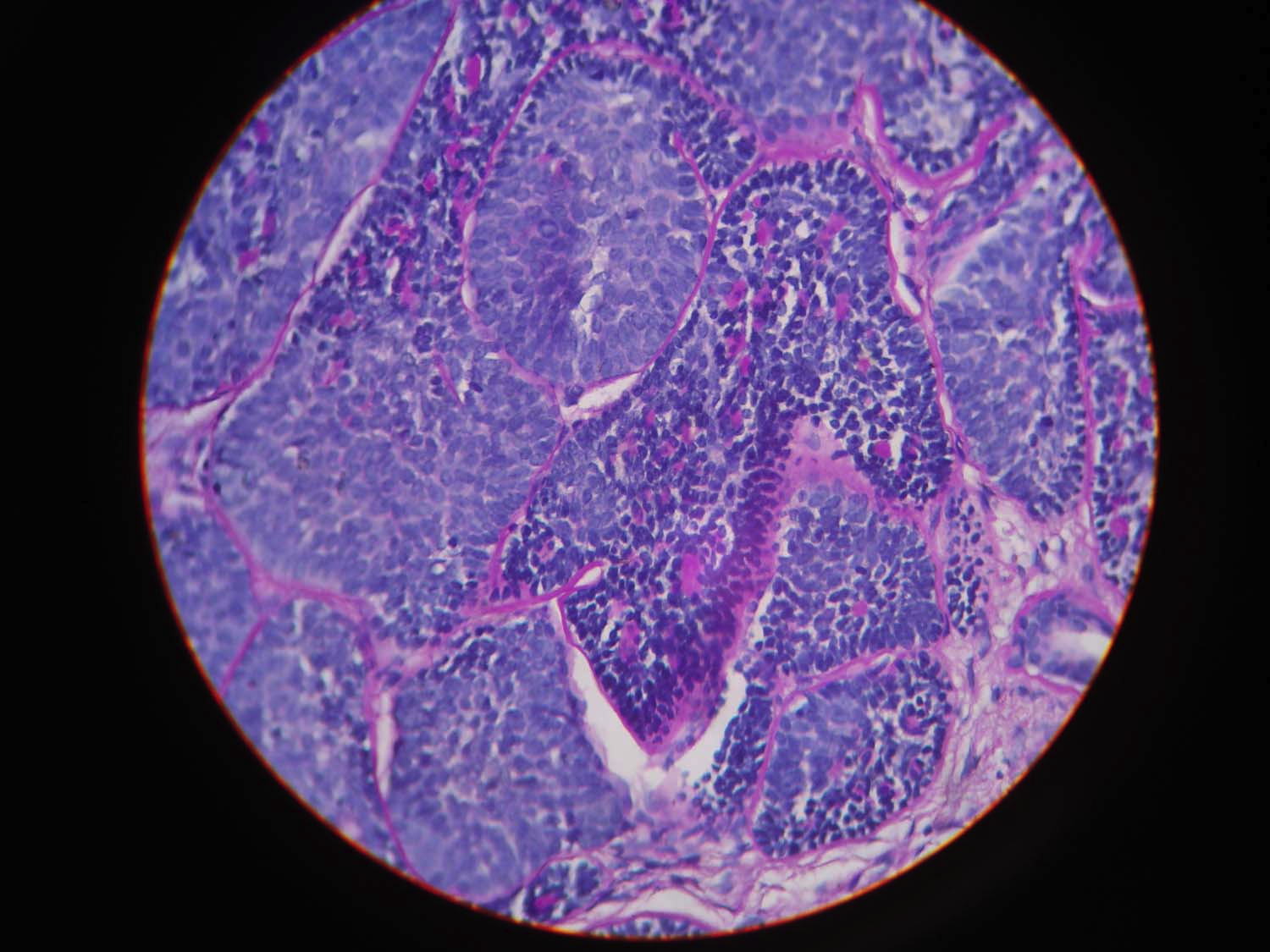
| Figure 6. Photomicrograph of cylindroma showing large lobulated nests of basaloid cells arranged in a jig-saw pattern (PAS x100) |
Punch biopsy from the facial lesion was performed in which the overlying epidermis was unremarkable and the dermis showed basaloid epithelial cell islands showing peripheral palisading along with horn cysts of varying sizes surrounded by a fibrous stroma (Figure 4) consistent with the diagnosis of trichoepithelioma. Shave excision biopsy from the scalp lesion was performed, which showed the overlying epidermis to be unremarkable. The dermis showed islands of basaloid cells arranged in an interlocking jig-saw puzzle like architecture (Figure 5). The islands were composed of two types of cells, the small dark cells arranged at the periphery and the larger lighter cells in the central area. These islands were surrounded by a thick hyalinized, periodic acid-Schiff staining basement membrane (Figure 6) consistent with cylindroma. On the basis of history, clinical presentation, and histopathological findings the diagnosis of Brooke-Spiegler syndrome was made.
Treatment
Various techniques have been used for the treatment of trichoepitheliomas and cylindromas including excision, electrocautery, carbon dioxide laser ablation, cryosurgery, and radiotherapy. In our case, radiofrequency ablation was used as a safe and economical treatment modality in the management of BSS. The result of treatment was also assessed on the basis of the perception of the patient. The patient was asked to rate the efficacy of treatment at various intervals on a scale of 0 to 100, i.e., visual analog scale. Resurfacing of the lesions was done in multiple sittings until they merged with the surrounding skin. This was taken as the endpoint of treatment.
 |  |
| Figure 7 | Figure 8 |
|---|---|
| Figure 7. Post treatment front view of face Figure 8. Posttreatment right lateral view of scalp and face | |
 |
| Figure 9 |
|---|
| Figure 9. Posttreatment left lateral view of face and scalp |
In our case, most of the cylindromas were pedunculated. The condition was explained to the patient. A single cylindroma was ablated with radiofrequency using cut and coagulation mode with power of # 2.5 to 3. Cosmetically acceptable results were achieved. Other cylindromas were also ablated by radiofrequency in multiple sittings.
Trichoepitheliomas were ablated using coagulation mode with power # 3 to 3.5. As the lesions were diffuse and scattered all over the face, they were ablated in multiple settings under local anaesthesia, followed by topical antibiotic (fusidic acid 2%). In 15 sittings, cosmetically acceptable results were achieved in 100 percent of the cylindromas and 70 percent of the trichoepitheliomas (Visual Analog Scale) as shown in Table 1 and Figures 7, 8, and 9.
Discussion
Brooke-Spiegler syndrome is an uncommon disease with a predisposition to develop cutaneous adnexal neoplasms such as cylindromas, trichoepitheliomas, spiradenomas, trichoblastomas, basal cell carcinomas, follicular cysts, and organoid nevi; malignant transformation of preexisting tumors in affected individuals is also seen [8]. Brooke-Spiegler syndrome results from mutations or loss of heterozygosity of the cylindromatosis gene (CYLD) located at 16q12-q13, which is a tumor suppressor gene [9, 10, 11, 12]. The most common tumors are cylindromas, trichoepitheliomas, and spidradenomas, which are typically located on the head and neck.
Various treatment modalities, which have been used successfully for cylindromas are excision, dermabrasion, electrodesiccation, CO2 laser, cryotherapy, and radiotherapy. Some treatment modalities such as dermabrasion and CO2 laser have high reoccurrence rates [13]. Some have supported wide local excision as the preferred treatment of choice to avoid risk of malignant transformation [14], but this gives cosmetically unacceptable results. The most common side effects of cryotherapy are hypopigmentation and depigmentation; these are often not acceptable on exposed sites. By electrodesiccation one can do only superficial diathermy, which is not very effective even after multiple sittings. If this modality is used deeply, it results in scarring, which is also not acceptable cosmetically. Recently, a therapeutic attempt has been made to treat single cylindromas in BSS with topically applied salicylic acid at varying concentrations. Salicylic acid acts by interfering with the NF-κB signaling pathway and is thought to be capable of blocking tumor progression and/or reducing the size of existing tumors. The results of this therapeutic approach are rather discouraging, however, probably because salicylic acid is a rather weak and nonspecific blocker of NF-κB activation. But previous data suggests that salicylic acid is not sufficiently potent to inhibit tumor growth [15]. Localized radiotherapy on exposed sites may cause radiation dermatitis resulting in decreased patient compliance. Coalescing trichoepitheliomas on the mid face have been successfully treated with the erbium:Yag laser [14]. These modalities are not widely accepted because of high costs. Moreover, radiofrequency ablation is a simple, safe procedure with wider applications. Savant et al, have concluded that radiofrequency ablation causes less lateral heat spread and tissue damage and provides better control in comparison to electrocautery [16, 17]. They have also described the cutting mode of radiofrequency as more effective and versatile in comparison to the carbon dioxide laser [17]. Because hemostasis occurs simultaneously, the time required for the surgery is less. There are fewer side effects and it is easy use. Therefore, we have used radiofrequency ablation in the treatment of both cylindromas and trichoepitheliomas. There were no clinical signs of recurrence in a 6 month follow up period. Hence, this technique is useful in the treatment of both trichoepitheliomas and cylindromas with well-accepted cosmetic results.
Conclusion
Brooke-Spiegler syndrome is a rare autosomal dominant inherited disease characterized by development of multiple trichoepitheliomas and cylindromas. We report a case of Brooke-Spiegler syndrome in which scalp cylindromas were treated with radiofrequency ablation under cut and coagulation mode. Trichoepitheliomas were treated under coagulation mode. Cosmetically acceptable results were 100 percent for the cylindromas and 70 percent for the trichoepitheliomas with no clinical signs of reoccurrence in a 6 month follow up period. The special features in our case are the coexistence of two adenexal tumors in a single patient and the positive family history in four generations. The radiofrequency ablation technique under different modes can be used in both large tumors as well as smaller ones. In developing countries it is very cost effective and easily accessible as proven by its second name “poor man’s laser.”
References
1. Ancell H. History of a remarkable case of tumours developed on the head and face; accompanied with a similar disease in the abdomen. Med Chir Trans. 1842;25: 227-246. [PubMed]2. Evans CD. Turban tumour. Br J Dermatol. 1954;66:434-43. [PubMed]
3. Gerretsen AL, Beemer FA, Deenstra W, et al. Familial cutaneous cylindromas: investigations in five generations of a family. J Am Acad Dermatol. 1995;33:199-206. [PubMed]
4. Poblete Gutierrez P, Eggermann T, Holler D, et al. Phenotypediversity in familial cylindromatosis: a frameshift mutation in the tumor suppressor gene CYLD underlies different tumors of skin appendages. J Invest Dermatol. 2002;119:527-31. [PubMed]
5. Massoumi R, Podda M, Fassler R, et al. Cylindroma as tumor of hair follicle origin. J Invest Dermatol. 2006;126:1182-4. [PubMed]
6. Young AL, Kellermayer R, Szigeti R, et al. CYLD mutations underlie Brooke-Spiegler, familial cylindromatosis, and multiple familial trichoepithelioma syndromes. Clin Genet. 2006;70:246-9. [PubMed]
7. Crain RC, Helwig EB. Dermal cylindroma (dermal eccrine cylindroma). Am J Clin Pathol. 1961;35:504-15. [PubMed]
8. Kazakov DV, et al. Brooke-Spiegler syndrome: report of a case with combined lesions containing cylindromatous, spiradenomatous, trichoblastomatous, and sebaceous differentiation. Am J Dermatopathol. 2005;27:27. [PubMed]
9. Ly H, Black MM, Robson A. Case of the Brooke-Spiegler syndrome, Australas J Dermatol. 2004 Nov;45(4):220-2. [PubMed]
10. Bignell GR, Warren W, Seal S, et al. Identification of the familial cylindromatosis tumour-suppressor gene. Nat Genet. 2000 Jun;25(2):160-5. [PubMed]
11. Trompouki E, Hatzivassiliou E, Tsichritzis T, et al. CYLD is a deubiquitinating enzyme that negatively regulates NF-kappa B activation by TNFR family members. Nature. 2003 Aug; 424(6950):793-6. [PubMed]
12. Biggs PJ, Wooster R, Ford D, et al. Familial cylindromatosis (turban tumour syndrome) gene localized to chromosome 16q12-q13: evidence for its role as a tumor suppressor gene. Nat Genet. 1995 Dec;11(4):441-3. [PubMed]
13. Gerretsen AL, van der Putte SCJ, Deenstra W, van Vloten WA. Cutaneous cylindroma with malignant transformation. Cancer. 1993 Sep;72(5):1618-23. [PubMed]
14. Rallan D, Harland CC. Brooke-Spiegler syndrome: treatment with laser ablation. Clin Exp Dermatol. 2005 Jul;30(4):355-7. [PubMed]
15. Brummelkamp TR, Nijman AMB, Dirac AMG, et al.Loss of the cylindromatosis tumour suppressor inhibits apoptosis by activating NF-kB. Nature. 2003; 424:797-801. [PubMed]
16. Hainer BL. Electrosurgery for the skin. Am Fam Physician. 2002;66:1259-66. [PubMed]
17. Savant SS. Radiosurgery. In : Savant SS, Gore D, Atal-Shah R, Sarangi K, editors. Textbook and atlas of dermatosurgery and cosmetology. 2nd ed. ASCAD: Mumbai, India; 2005. p. 305-14.
© 2012 Dermatology Online Journal