Ulcerated plaque under a ruby ring in an immunosuppressed patient
Published Web Location
https://doi.org/10.5070/D32jb121rbMain Content
Ulcerated plaque under a ruby ring in an immunosuppressed patient
Elizabeth RC Geddes MD MSc1, Kristel Polder MD2, Jonathan E Cutlan MD3, Carlos A Torres-Cabala MD4, Sharon R Hymes MD5
Dermatology Online Journal 16 (8): 4
1. The University of Texas Medical School at Houston, Houston, Texas. Elizabeth.R.Geddes@uth.tmc.edu2. Suzanne Bruce and Associates, Houston, Texas
3. Dermatopathology Fellow, Department of Pathology, The University of Texas M.D. Anderson Cancer Center, Houston, Texas
4. Department of Pathology, The University of Texas M.D. Anderson Cancer Center, Houston, Texas
5. Department of Dermatology, The University of Texas M.D. Anderson Cancer Center, Houston, Texas
Abstract
We report a primary inoculation fungal infection in a 76-year-old man with acute myeloid leukemia. The patient presented with a painful red plaque located where he routinely wore a ruby ring. Histopathology revealed multiple branching septate hyphae. Cultures confirmed Fusarium and Candida parapsilosis infection. A short discussion of these organisms follows.
Introduction
Primary cutaneous non-dermatophyte fungal infections are unusual and result from the direct inoculation of spores into injured skin. The organisms most likely to cause a local cutaneous infection include Aspergillus, Fusarium, Mucor, and Rhizopus species [1]. There is a risk of subsequent deep tissue invasion and dissemination in severely neutropenic patients, such as those with hematologic malignancies undergoing chemotherapy or bone marrow transplantation [2]. Here we present a case of primary inoculation cutaneous Fusarium and Candida parapsilosis infection from wearing a ruby ring.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Erythematous plaque with central dusky erosion and dark black crust on the dorsal aspect of the right fourth finger. Figure 2. Underside of the ruby ring worn prior to the infection. | |
A 76-year-old man with newly diagnosed acute myeloid leukemia was admitted for induction/consolidation chemotherapy with clofarabine and low-dose cytarabine. Four days prior, the patient developed a lesion on his right fourth digit, directly underneath the pointed tip of a routinely worn ruby ring (Figure 1). The lesion became increasingly tender and the ring became painful to wear. He also reported that a whitish substance seemed to be growing on the ring’s undersurface for several weeks prior to the development of the lesion (Figure 2). He denied any fever, chills, dyspnea, cough, or other cutaneous lesions. The remainder of the review of systems was negative.
 |  |
| Figure 3 | Figure 4 |
|---|---|
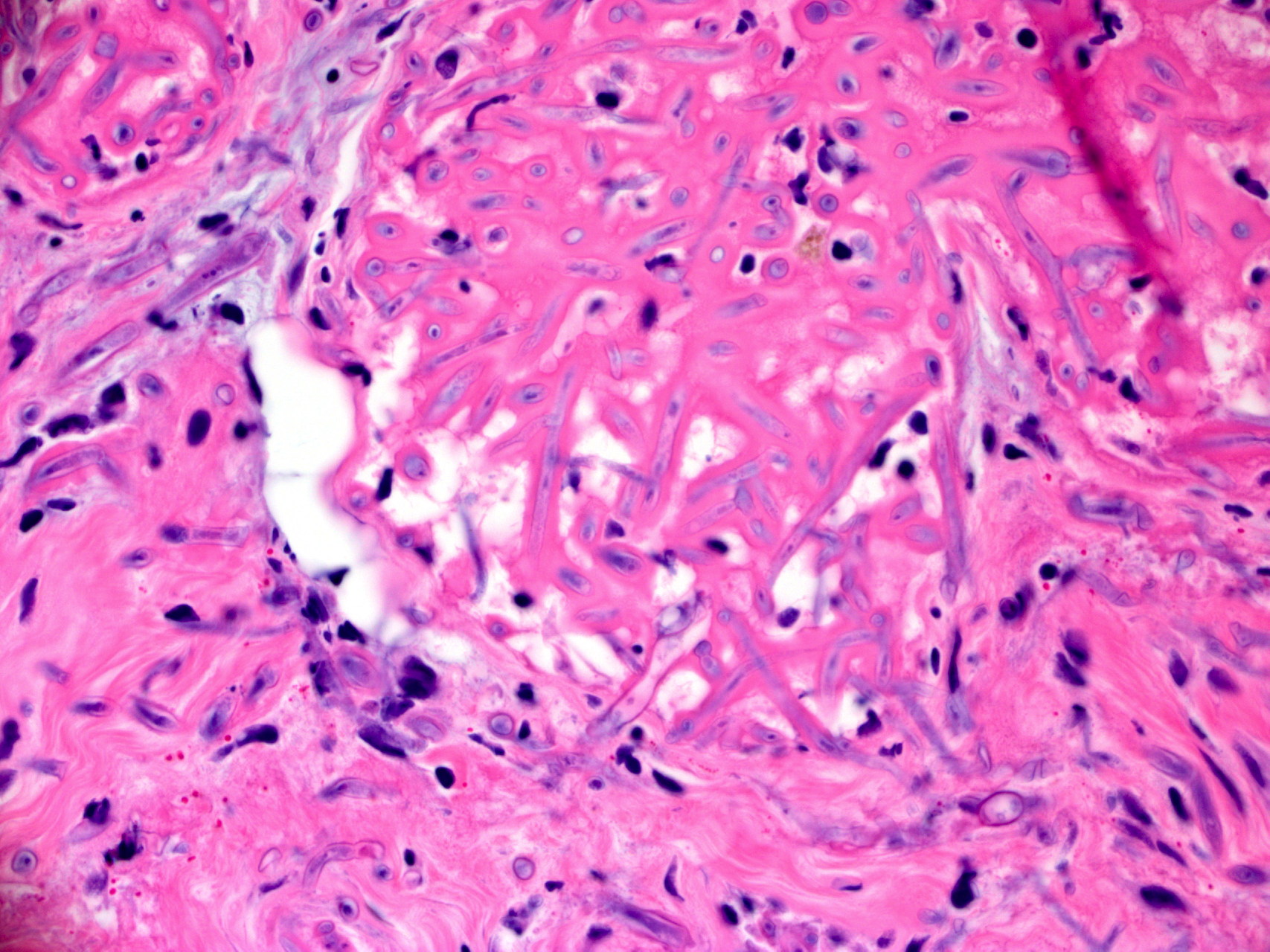
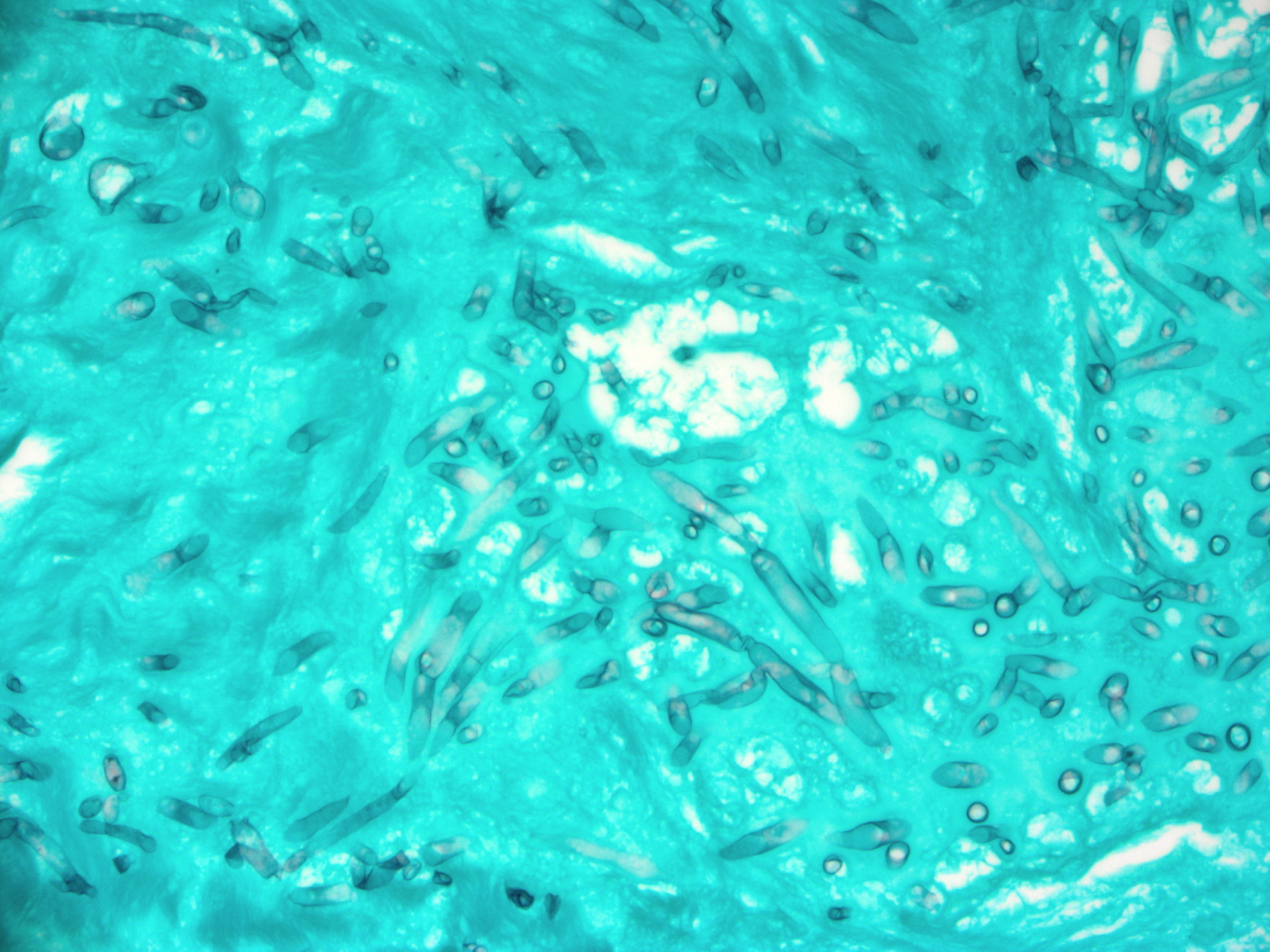
| Figure 3. Septated fungal branching hyphae in the dermis invading blood vessels. (H&E, x60) Figure 4. Septated fungal branching hyphae (Gomori Methenamine Silver [GMS] stain, x60) | |
Physical exam revealed a 1 cm erythematous plaque on the dorsal aspect of the right fourth finger, with a central dusky eschar corresponding to the pointed tip of the ruby. The surrounding skin was erythematous and edematous. A skin biopsy was performed and sent for frozen section, tissue culture, and hematoxylin and eosin staining. Swab culture of the undersurface of the ring was also taken. Histopathology revealed abundant septate fungal hyphae in the dermis with evidence of intravascular involvement (Figures 3 and 4). Cultures of the wound and material growing under the ring grew Candida parapsilosis and Fusarium species.
Discussion
Fusarium species are filamentous fungi with septate hyaline hyphae found in soil. Most primary localized Fusarium infections of the skin occur on the distal extremities, especially the hands and feet [3]. Any area of epidermal compromise can potentially become infected by Fusarium in high-risk patients, including locations of indwelling catheters, surgical or traumatic wounds, and even insect bites [3]. The lesions are often subcutaneous nodules or ecthyma gangrenosum-like with a black eschar [2], which reflects the organism’s propensity for vascular invasion and cutaneous necrosis [1]. Biopsy and culture are required to confirm Fusarium infection, because it is difficult to distinguish from Aspergillus by routine histology. Voriconazole, posaconazole, or itraconazole may be effective oral antifungal therapy. Extensive surgical debridement may be required [3]. Recovery from neutropenia is often crucial to overcome infection [1, 3].
Candida parapsilosis, the second organism isolated, is one of the most common non-albicans Candida species. Risk factors for primary infection include foreign body or line insertion [4].
Reports of jewelry and resultant infection of the wearer are uncommon and largely limited to accessories that involve a break in the epidermal barrier, such as body piercings [5]. We speculate that the point on the ruby gemstone in the ring traumatized the underlying skin, allowing a portal of entry for the fungal species, which were already growing around the stone. This report illustrates the necessity of performing thorough skin surveillance in immunocompromised patients. Any jewelry that could possibly serve as a nidus of infection should be removed.
References
1. Mays SR, Bogle MA, Bodey GP. Cutaneous fungal infections in the oncology patient: Recognition and management. Am J Clin Dermatol 2006;7:31-43. [PubMed]2. Boutati EI, Anaissie EJ. Fusarium, a significant emerging pathogen in patients with hematologic malignancy: ten years’ experience at a cancer center and implications for management. Blood 1997;90(3):999-1008. [PubMed]
3. Bodey GP, Boktour M, Mays S, Duvic M, Kontoyiannis D, Hachem R, Raad I. Skin lesions associated with Fusarium infection. J Am Acad Dermatol 2002;47:659-666. [PubMed]
4. Krcmery V, Barnes AJ. Non-albicans Candida spp. causing fungaemia: pathogenicity and antifungal resistance. Journal of Hospital Infection 2002;50:243-260. [PubMed]
5. Tweeten SM, Rickman LS. Infectious complications of body piercing. Clinical Infectious Disease 1998;26:735-740. [PubMed]
© 2010 Dermatology Online Journal