Neutrophilic eccrine hidroadenitis with atypical findings
Published Web Location
https://doi.org/10.5070/D32g73v82nMain Content
Letter: Neutrophilic eccrine hidroadenitis with atypical findings
Emiliano Grillo MD, Sergio Vano-Galvan, Carmen Gonzalez, Jaén Pedro
Dermatology Online Journal 17 (9): 14
Hospital Ramón Y Cajal, Madrid, Madrid, SpainAbstract
Neutrophilic eccrine hidradenitis (NEH) was originally described as a distinctive dermatosis occurring in patients undergoing chemotherapy, especially associated with the use of cytarabine in the treatment of acute myelogenous leukemia (AML). This disorder is characterized by a neutrophilic infiltrate around the eccrine glands and coils and is associated with necrosis. However, atypical findings in the histology have been reported. To the best of our knowledge, leukocytoclastic vasculitis has not been described in association with NEH. We hypothesize that a toxic effect of cytarabine may damage the vessel wall to some extent, causing a vasculitic phenomenon.
Introduction
Neutrophilic eccrine hidradenitis (NEH) is a reactive disorder that may occur in association with malignancy (with or without chemotherapy), infections, certain medications, or even in healthy individuals [1].
Acute myeloid leukemia and treatment with cytarabine are the most frequently associated situations [2].
The clinical lesions are typically erythematous and edematous plaques that may be purpuric and painful. They are usually located on the extremities, trunk, face, and palms, and may mimic cellulitis when appearing around the eyes.
A skin biopsy demonstrating typical pathologic changes of the eccrine glands is required to confirm a diagnosis of NEH. It is characterized by a neutrophilic infiltrate around the eccrine glands and coils and is associated with necrosis. We report a case of NEH associated with leukocytoclastic vasculitis on histology. To our knowledge, leukocytoclastic vasculitis has not been reported in association with NEH.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Clinical image of the patient presenting with high fever and painful erythematous lesions on the eyelids Figure 2. Clinical image of the patient showing painful erythematous and infiltrated plaques on the left breast | |
A 37-year-old woman was admitted with headache and pancytopenia and was diagnosed with acute myeloid leukemia, French-American-British (FAB) subtype 1. She developed fever (39°C) on the seventh day of admission.
Concomitantly, she developed symmetrical, erythematous plaques, predominantly in a periorbital distribution and over the left breast. The lesions consisted of well-demarcated, erythematous, and edematous plaques that were tender on palpation (Figures 1 and 2).
Clinically the differential diagnosis included dermatomyositis, acute febrile neutrophilic dermatosis, and infectious process.
Empirical antimicrobial therapy using intravenous piperaciline-tazobactam was started. Extensive screening found no infectious cause for her pyrexia. Two skin biopsies of the cutaneous lesions over the left breast and the left lower eyelid were performed.
 |  |
| Figure 3 | Figure 4 |
|---|---|
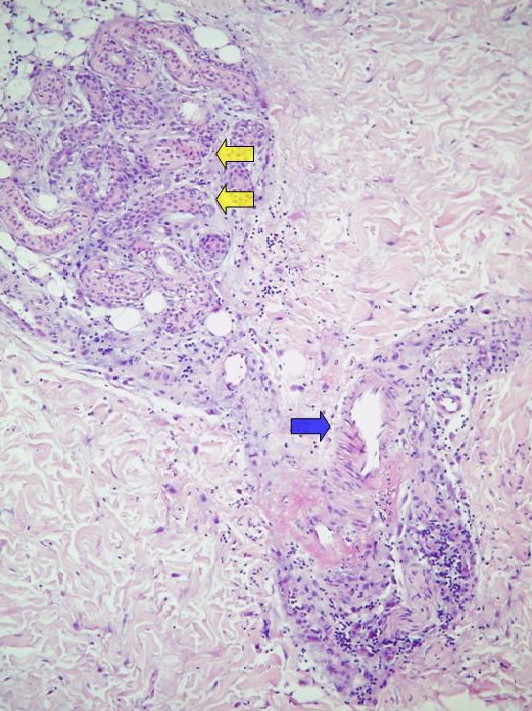
| Figure 3. Biopsy of lesions located on the breast showed a neutrophilic infiltrate with vacuolar degeneration around the eccrine
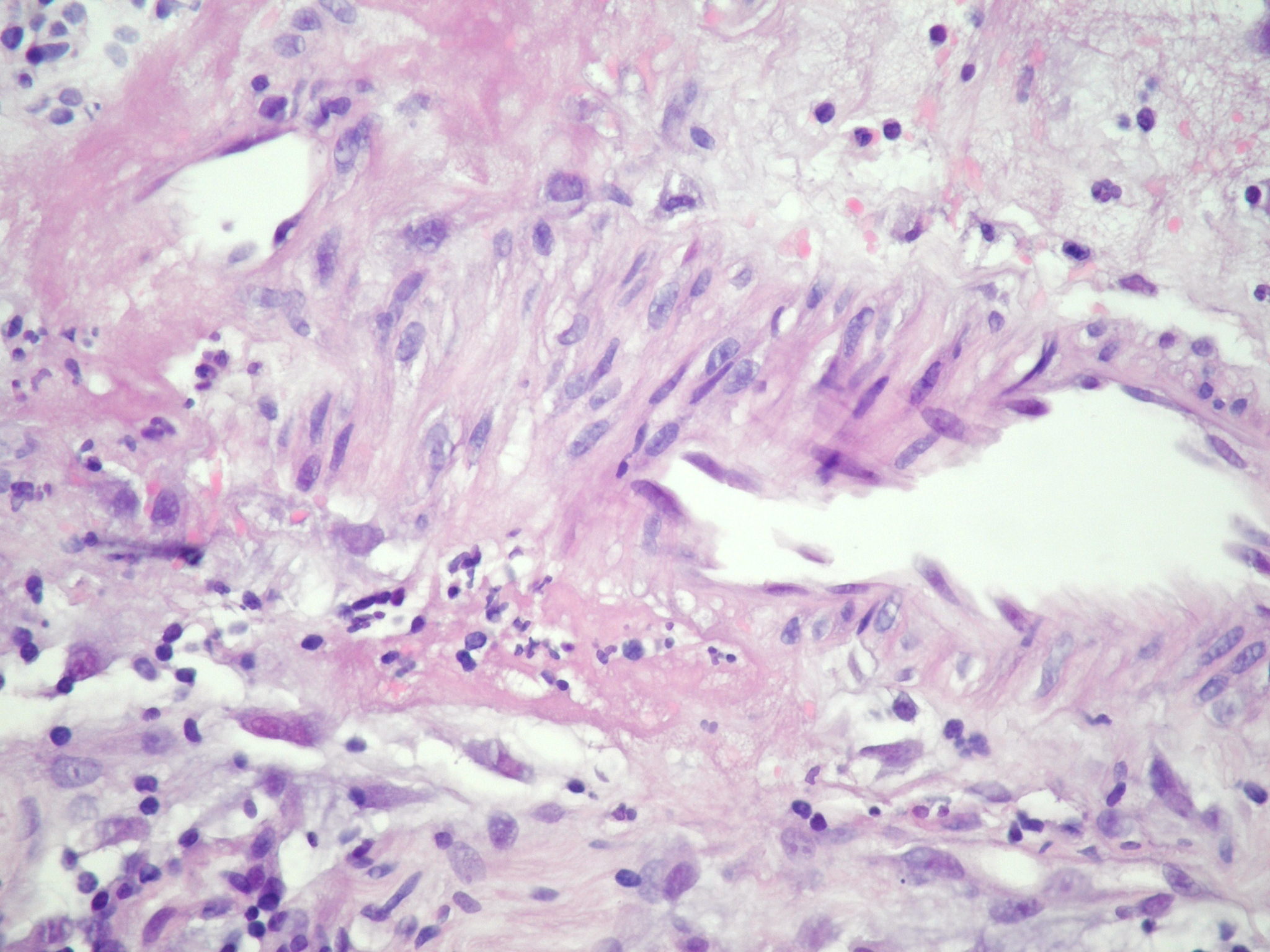
glands (yellow arrows) associated with findings of leukocytoclastic vasculitis (blue arrow; H&E, x10). Figure 4. High power view of leukocytoclastic vasculitis: We can see a neutrophilic infiltrate and fibrinoid necrosis. | |
 |
| Figure 5 |
|---|
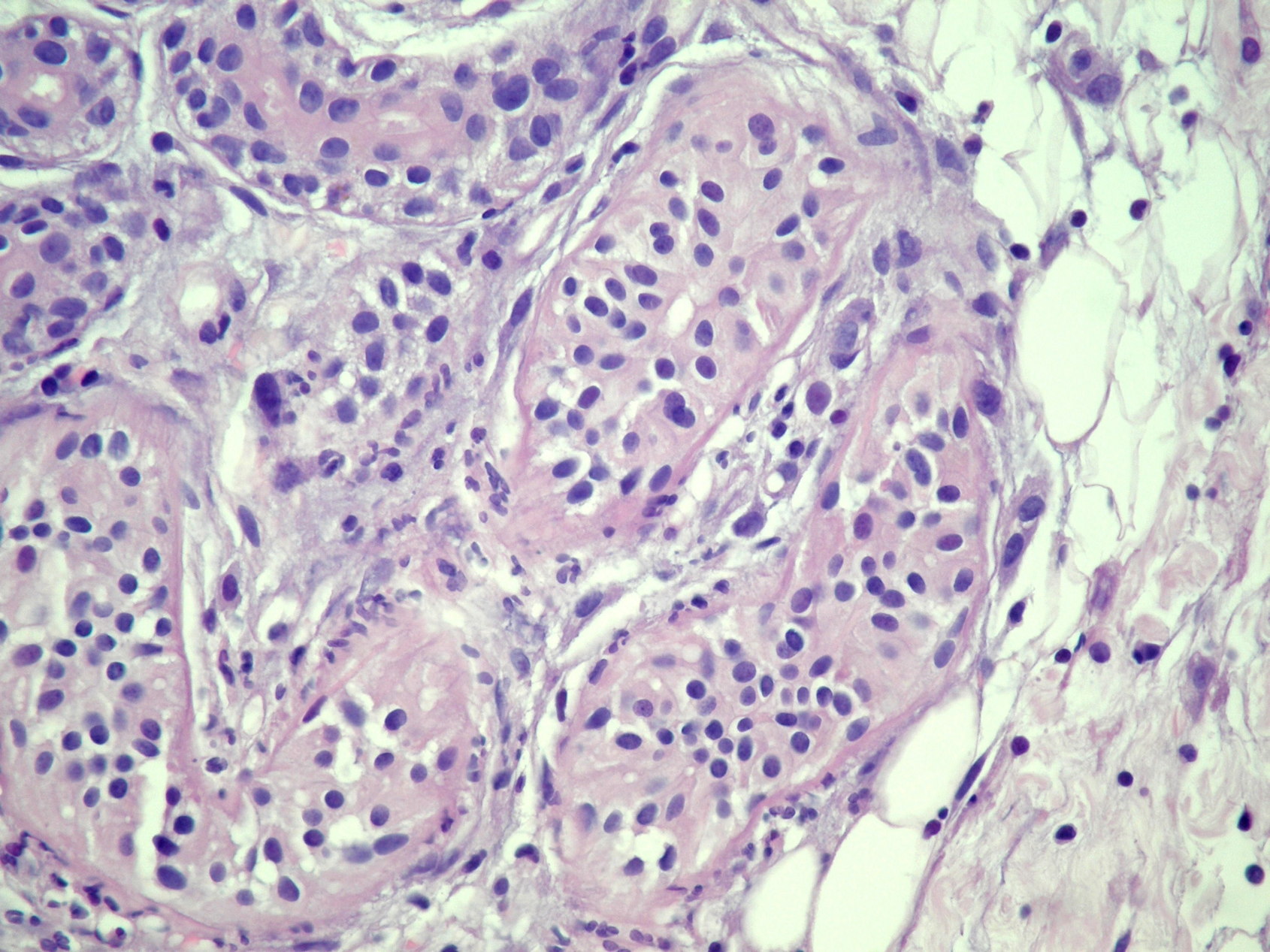
| Figure 5. Enlarged image of the eccrine glands: There is an infiltrate of neutrophils around and within the eccrine secretory coils, associated with vacuolar degeneration. The neutrophilic infiltrate may be mild in patients with neutropenia (H&E, x40). |
Histological features of the eyelid biopsy consisted of a neutrophilic infiltrate surrounding the eccrine glands and sparing the duct. There was a focal interface vacuolar dermatitis. Biopsy of lesions located on the breast showed a neutrophilic infiltrate around the eccrine glands associated with findings of leukocytoclastic vasculitis (Figures 3, 4, and 5). An ill-defined collection of histiocytes, large and pleomorphic, and scattered lymphocytes could be observed within the dermis and subcutaneous tissue. Based on the clinical and histological findings a diagnosis of NEH secondary to cytarabine was made.
A trial of topical corticosteroids was initiated. The fever settled over the next 3 days and the skin lesions resolved gradually with post-inflammatory hyperpigmentation.
Discussion
Most cases of NEH have been reported as a rare toxic reaction in patients treated with different chemotherapeutic regimens for acute myelogenous leukemia or other hematologic malignancies. However, other associations have been recognized in addition to chemotherapeutic agents, including Behçet disease, human immunodeficiency virus (HIV) infection, staphylococcus or streptococcus infections, and hemodialysis [3, 4, 5, 6].
The pathogenesis of NEH is unclear. Two major hypotheses have been proposed in the literature. First, NEH may be the consequence of a direct toxic effect of a drug secreted in the sweat from eccrine coils and duct cells. This may ultimately be shown to account for many of the chemotherapy-related cases [7]. More than 70 percent of oncology patients who develop NEH do so after their first course of chemotherapy. In contrast, other investigators have postulated that NEH is a hypersensitivity reaction within the spectrum of neutrophilic dermatosis such as Sweet syndrome. The observation that NEH may occur in patients with no previous treatment supports this hypothesis [8, 9].
A biopsy is required to establish the diagnosis. Because NEH usually occurs in the context of febrile neutropenia, culture of tissue specimens is mandatory before the diagnosis of NEH is established. Routine biopsy specimens reveal a dense neutrophilic infiltrate within and around eccrine glands, which may be accompanied by necrosis of eccrine epithelial cells. Some severely neutropenic patients may have a paucity or absence of neutrophils histologically, but the necrosis of eccrine glands is evident. Apocrine gland involvement, squamous syringometaplasia, dermal hemorrhage, dermal edema, epidermal spongiosis, basal vacuolization, focal keratinocyte necrosis, mucin deposits, and mild, superficial panniculitis may be observed [10].
To the best of our knowledge, leukocytoclastic vasculitis has not been reported in association with NEH. We hypothesize that the toxic effect of cytarabine in our case may have altered the vessel wall, causing a vasculitic phenomenon. La relación temporal de la patología cutánea con la introducción del fármaco apoya esta teoría.
In conclusion, we should consider vasculitis as another possible coexisting phenomenon in cases of NEH secondary to cytarabine.
References
1. Manganoni AM, Facchetti F, Gavazzoni R, Marocolo D, De Panfilis G: Neutrophilic eccrine hidradenitis in a healthy woman. Dermatology 1994; 189: 211-212. [PubMed]2. Harrist TJ, Fine JD, Berman RS, Murphy GF, Mihm MC Jr: Neutrophilic eccrine hidradenitis. A distinctive type of neutrophilic dermatosis associated with myelogenous leukemia and chemotherapy. Arch Dermatol 1982; 118: 263-266. [PubMed]
3. Mercader-García P, Vilata-Corell JJ, Pardo-Sanchez J, et al. Neutrophilic eccrine hidradenitis in a patient with Behçet’s disease. Acta Derm Venereol 2003; 83: 395-396. [PubMed]
4. Bachmeyer C, Reygagne P, Aractingi S. Recurrent neutrophilic eccrine hidradenitis in an HIV-1-infected patient. Dermatology 2000; 200: 328-330. [PubMed]
5. Shih IH, Huang YH, Yang CH, et al. Childhood neutrophilic eccrine hidradenitis: a clinicopathologic and immunohistochemical study of 10 patients. J Am Acad Dermatol 2005; 52: 963-966. [PubMed]
6. Takai T, Matsunaga A. A case of neutrophilic eccrine hidradenitis associated with streptococcal infectious endocarditis. Dermatology 2006; 212: 203-205. [PubMed]
7. Bachmeyer C, Aractingi S. Neutrophilic eccrine hidradenitis. Clin Dermatol 2000; 18: 319-330. [PubMed]
8. Kuttner BJ, Kurban RS. Neutrophilic eccrine hidradenitis in the absence of an underlying malignancy. Cutis 1988; 41: 403-405. [PubMed]
9. Smith KJ, Skelton HG 3rd, James WD, et al. Neutrophilic eccrine hidradenitis in HIV-infected patients. J Am Acad Dermatol 1990; 23: 945-947. [PubMed]
10. Bailey, D.L, Barron, D., Lucky, A.W. Neutrophilic eccrine hidradenitis: a case report and review of the literature. Pediatr Dermatol 1989; 6: 33-38. [PubMed]
© 2011 Dermatology Online Journal