Clinico-histopathological correlation and the treatment response of 20 patients with cutaneous tuberculosis
Published Web Location
https://doi.org/10.5070/D324s2k2xhMain Content
Letter: Clinico-histopathological correlation and the treatment response of 20 patients with cutaneous tuberculosis
Ranthilaka R Ranawaka MD1, Priyanka H Abeygunasekara MD2, Eshanth Perera MD3, Hema S Weerakoon MBBS1
Dermatology Online Journal 16 (8): 13
1. Department of Dermatology2. Department of Pathology
3. Department of Respiratory Medicine
Teaching Hospital Anuradhapura, Sri Lanka
Abstract
Cutaneous tuberculosis (TB) can mimic other granulomatous diseases clinically and histopathologically. This case series relates images and workup of 20 patients who were histopathologically and therapeutically confirmed to have cutaneous TB. Although positive results of ESR, Mantoux reactivity, and TB cultures facilitate the clinical diagnosis, negative results should not exclude the diagnosis of cutaneous TB. An alternative cause should be considered if the clinical response to anti-TB drugs is inapparent within 2 months.
Introduction
Approximately 7000 to 8500 new tuberculosis (TB) cases are detected annually and still continue to be a major health issue in Sri Lanka. In 2007, a total of 8497 patients were diagnosed with tuberculosis and 1984 (23.3%) of these were in extrapulmonary sites. The annual risk of TB incidence at the national level remains 1.8 percent.
Several published studies have revealed that cutaneous TB is best diagnosed using a comprehensive work up of the patient in which histologic study of the skin biopsy specimen is most essential. Mantoux reactivity, TB culture, or the erythrocyte sedimentation rate (ESR) were not reliable in diagnosis [1-6]. Polymerase chain reaction (PCR) has emerged as a promising tool in the diagnosis of cutaneous TB and atypical mycobacteria infections [7-12]. More recently, a new diagnostic method, interferon-gamma enzyme-linked immunosorbent assay (QuantiFERON TB-gold in tube, (QFT-2G), has been developed to detect latent tuberculosis infection. From a clinical trial of QFT-2G in which the subjects were smear-positive, untreated TB patients and BCG-vaccinated healthy individuals, it has been demonstrated that the specificity and sensitivity of QFT-2G are 98.1 percent and 89.0 percent, respectively, and that QFT-2G is an excellent diagnostic method [13, 14].
This case series was retrospectively gathered to emphasize the importance of clinicohistopathological correlation and therapeutic response in confirming cutaneous TB.
Patients and methods
In 32 patients who were clinically suspected of having cutaneous TB, tuberculoid granulomata were identified histologically (Figure 1). Full blood count, ESR, Mantoux test, HIV screening test, and leishmania slit-skin-smear were performed. Tuberculosis culture and PCR were performed on selected patients because these facilities were not available locally. Chest X-ray was performed prior to therapy to exclude pulmonary involvement. Except for thorough history and physical examination, and routine blood count and biochemistry tests, investigations to exclude extra-pulmonary TB were not performed. All patients were Human Immunodeficiency Virus (HIV) negative.
Diagnosed patients were treated with first line anti-TB drugs (CAT1) for 6 months: i.e. isoniazid(H) 10mg/kg, rifampicin(R) 10mg/kg, pirazinamide(Z) 30mg/kg and ethambutol(E) 15mg/kg (HRZE). All 4 drugs were given for the first two months, followed by isoniazid and rifampicin for the next four months. Second line anti TB drugs (CATII) for 8 months were given to one patient, i.e., HRZE plus intramuscular streptomycin 500 mg to 1 g daily for 60 days, followed by HRZE for 1 month and HR for another 5 months.
Case series
Twenty patients had histopathologically and therapeutically confirmed cutaneous TB; twelve were with Lupus Vulgaris (LV) and eight with Tuberculosis Verrucosa Cutis (TVC). See Table 1 and Table 2.
 |
| Figure 1 |
|---|
| Figure 1. Cutaneous Tuberculosis in Anuradhapura, Sri Lanka: distribution of patients and summary of results |
The average age of our study group was 35.2 years, ranging from 2.5 to 61 years; 3(15%) were children aged 2.5, 9, and 16 years. Mean delay in presentation was 2.4 years, ranging from 4 months to 20 years.
Lupus vulgaris (LV) presented as two clinical forms:
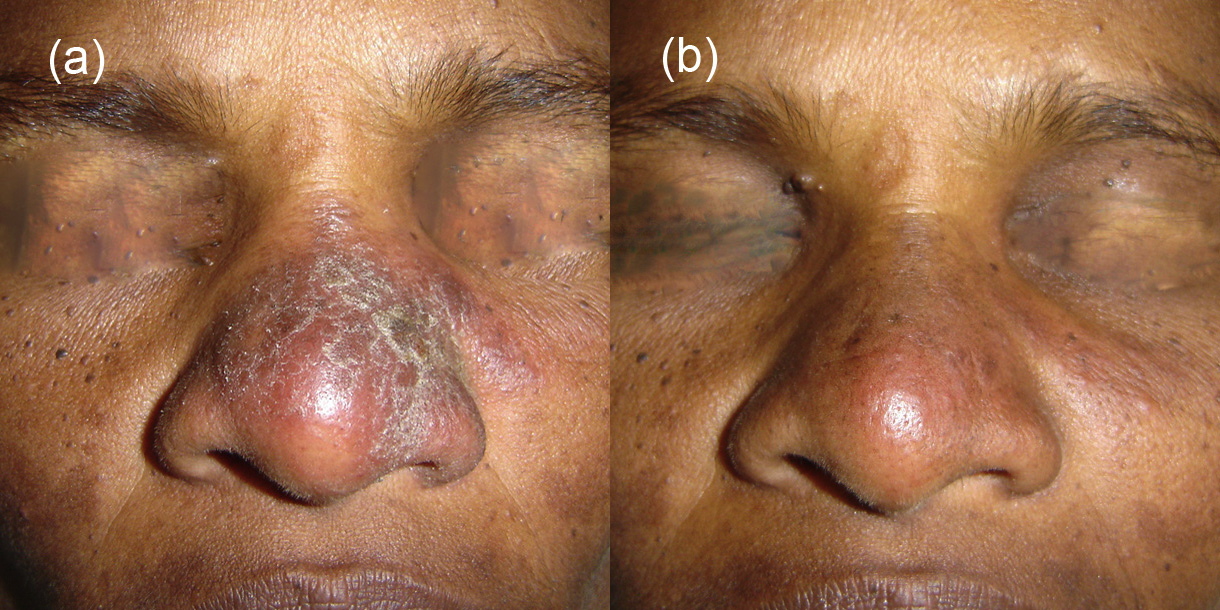
1. There were 8 patients with asymptomatic, erythematous or skin colored plaques. They were usually solitary (n=6), soft plaques of 0.5-4 cm diameter, located on the face (n=7) and back of calf (n=1). These clinically resembled tuberculoid leprosy, cutaneous leishmaniasis, and cutaneous sarcoidosis (Figure 2 - Patient 1).
2. There were 4 patients with plaques of 5 to 40 cm on the trunk (n=3) and hand (n=1), which were atrophic and scarred at the center with an irregular, erythematous, raised, active edge with peripheral extension (Figure 3 - Patient 9, Figure 4 - Patient 10). These clinically resembled late lesions of chromomycosis.
Tuberculosis Verrucosa Cutis (TVC) presented as a solitary warty lesion on feet (n=5), dorsum of hand (n=2), knee (n=2), and finger (n=1); the size ranged from 1-6 cm in diameter. In these cases the differential diagnosis was early lesion of chromomycosis, viral wart, fish tank granuloma (Mycobacterium marinum), and carcinoma (Figure 5 and Figures 8 through 10 - Patients 16-19).
 |  |
| Figure 2 | Figure 2c |
|---|---|
| Figure 2. Patient 1 a 40-year-old woman with lupus vulgaris (a) before treatment, (b) complete resolution of the lesion without a scar after 2 months of CAT I (c) after 6 months. | |
 |  |
| Figure 3 | Figure 3c |
|---|---|
| Figure 3. Patient 9 a 61-year-old man with lupus vulgaris (a) before treatment, (b) good clinical response after 2 months, and (c) complete resolution of the lesion leaving a scar after 6 months of CAT1 | |
 |  |
| Figure 4 | Figure 5 |
|---|---|
| Figure 4. A 48-year-old woman (Patient 10) who was on oral dexamethasone pulse for 2 years for her mixed connective tissue
disease, with lupus vulgaris (a) before treatment, (b) complete resolution of the lesion with a scar after 5 months of anti
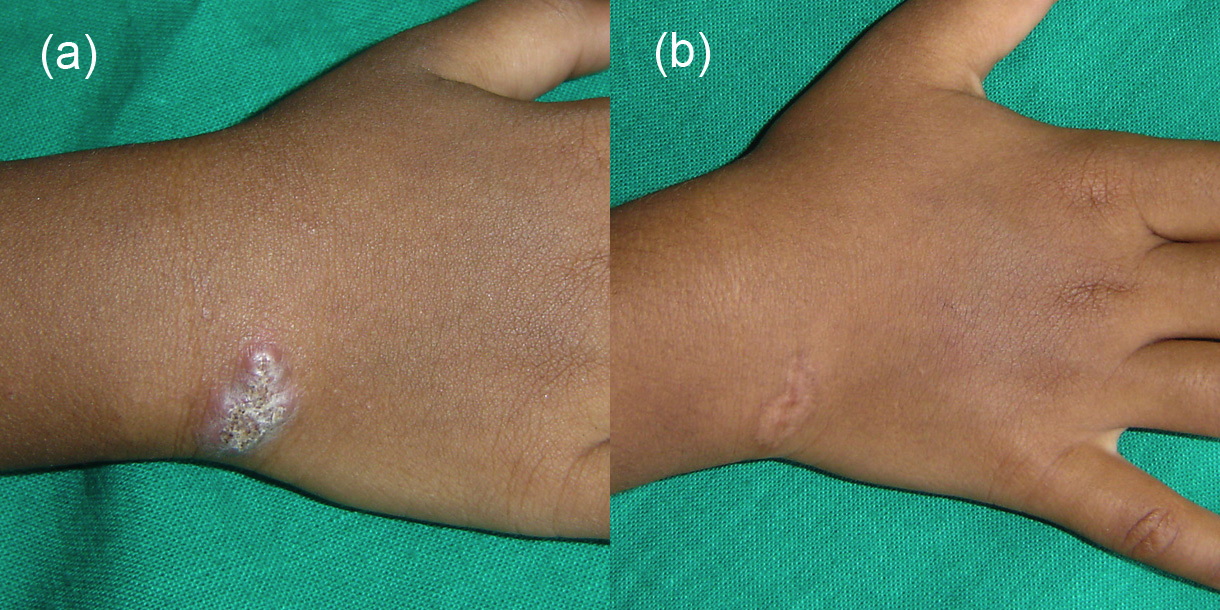
tuberculosis therapy Figure 5. The youngest patient in our case series, a 2½-year-old child (patient 16) with tuberculosis verrucosa cutis on right hand (a) before treatment, (b) complete resolution of the lesion after 2 months. | |
Information regarding Mantoux reactivity was available in 14: These showed ≥10mm diameter (positive) in 5 and <10mm diameter (negative) in 9. TB cultures were done on 6 and were negative in all. Lupus vulgaris showed classical tuberculous histology with unremarkable epidermis and upper dermis containing granulomata composed of collections of epithelioid cells, Langerhan type giant cells, histiocytes, and a moderate infiltrate of lymphocytes (Figures 6 and 7). None of the histology sections showed caseation necrosis. TVC showed epidermis with hyperkeratosis, acanthosis, papillomatosis, or pseudo-epitheliomatous hyperplasia and dermis with classical tuberculous histology without caseation. Ziehl-Neelson stain was not performed routinely.
None had pulmonary TB at present or past.
 |  |
| Figure 6a | Figure 6b |
|---|---|
| Figure 6. Classical tuberculous histology with unremarkable epidermis and upper dermis containing granulomata composed of collections of epithelioid cells, Langerhan type giant cells, histiocytes and moderate infiltrate of lymphocytes without caseation. (H&E, x10) | |
 |  |
| Figure 7 | Figure 8 |
|---|---|
| Figure 7. Cutaneous tuberculosis. (H&E, x40) Figure 8. Patient 17, a 25-year-old woman with (a) tuberculosis verrucosa cutis on left index finger, (b) reduced in size after skin biopsy. | |
Two patients (10%) noticed marked reduction of the lesion after skin biopsy (Figure 8 - Patient 17). Total disappearance of the skin lesions was noted within 2 months of anti-TB therapy in 16 (80%). All completed 6 months of CAT1 irrespective of early clinical response.
 |  |
| Figure 9 | Figure 9c |
|---|---|
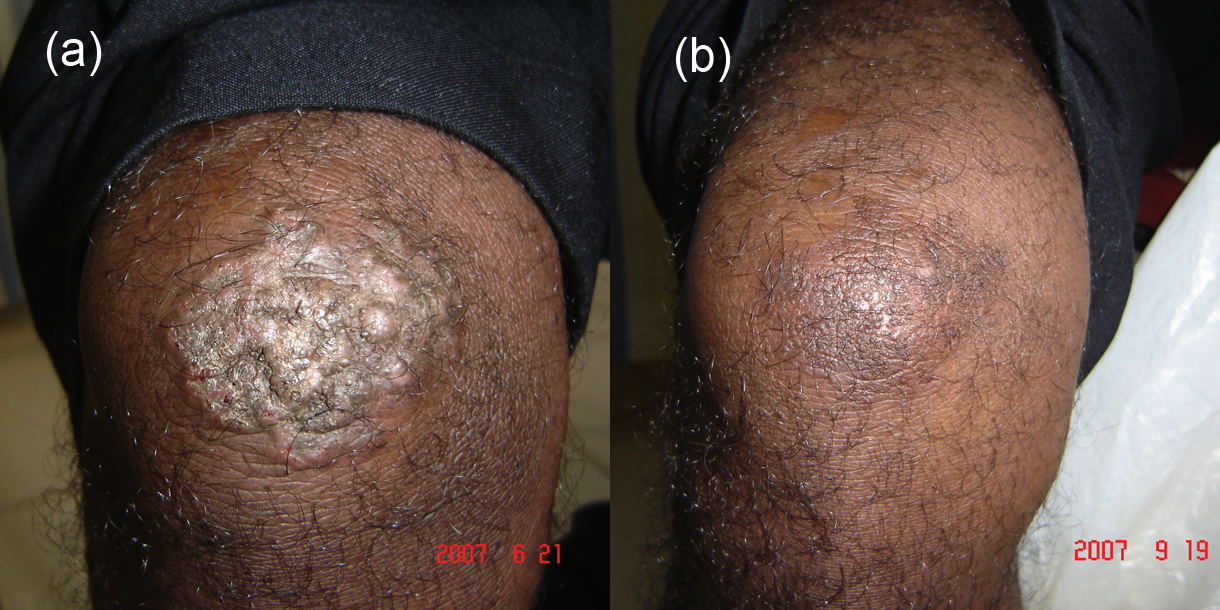
| Figure 9. Patient 18, a 33-year-old man with warty TB on knee (a) before therapy, (b) good clinical response after 3 months, and (c) complete resolution of the lesion without a scar after 6 months of anti tuberculosis therapy. | |
 |  |
| Figure 10 | Figure 11 |
|---|---|
| Figure 10. A 16-year-old boy (Patient 19) with warty TB on knee showed good clinical response within 2 months and the lesion
totally disappeared in 4 months. Figure 11. A 52-year-old man (Patient 12) with lupus vulgaris (a) after 3 months of anti-TB therapy, (b) partial clinical response after completion of 6 months anti tuberculosis therapy. | |
A 59-year-old farmer who did not respond to CAT1 was further investigated. Occasional “copper pennies” were identified in deep sections of a repeat skin biopsy to confirm a diagnosis of chromomycosis (Figure 13, Figure 13a, and Figure 13b).
 |  |
| Figure 13 | Figure 13a |
|---|---|
| Figure 13. A 59-year-old farmer was initially diagnosed with lupus vulgaris on histopathology, but did not respond to 6 months
of anti TB therapy (CAT1). Deep sections in a repeat skin biopsy showed occasional copper pennies that confirmed a diagnosis
chromomycosis. The lesion responded to a combination of oral itraconazole and liquid nitrogen cryotherapy. Figure 13. Chromomycosis: (a) granulomatous response and arrow shows the spores (H&E, x10), (b) Chromo spores in higher magnification (H&E, x40) | |
 |
| Figure 13b |
|---|
The Patient 10 (Figure 4) was on oral dexamethasone pulse for two years for her uncontrolled mixed connective tissue disease. Patient 16 (Figure 5) was given BCG vaccination twice, at birth and at 6 weeks of age, but had not developed the BCG scar. Except this patient, all had BCG vaccination at birth and had visible scar. Human immunodeficiency virus screening was negative in all.
An injured army soldier related the skin nodules to sand implantation in skin during a blast injury in 1999 (Figure 12). His ESR was 80 mmh1, HIV screening test, leishmania smear test, Mantoux test and TB cultures were negative twice. He did not respond to CATI or CATII and was lost to follow-up.
 |
| Figure 12 |
|---|
| A 32-year-old army soldier with an amputated left leg following a blast injury in 1999 presented with TB lymphadenitis in 2007. On anti-TB drugs (CATI) he developed numerous skin nodules of 0.5-1 cm diameter on the back of both forearms and thighs, which were histopathologically reported as mycobacterial infection. |
Discussion
Lupus vulgaris was the most common clinical manifestation in our case series. The most common site of LV was the face (58.3%), which generally healed without significant residual scarring. Other manifestations of cutaneous TB such as scrofuloderma, tuberculous gumma, orificial TB, acute miliary TB, and tuberculids were not seen in our study group and are seldom seen in Sri Lanka [15, 16, 17, 18].
Cutaneous TB can mimic other granulomatous diseases (cutaneous leishmaniasis, tuberculoid leprosy, superficial granulomatous pyoderma, cutaneous sarcoidosis, lupus miliaris disseminatus faciei, and chromomycosis) clinically and histopathologically as seen in our case series (Figures 13 through 15).
 |  |
| Figure 14 | Figure 15 |
|---|---|
| Figure 14. A 15-year-old girl presented with asymptomatic erythematous papules and nodules on the right leg with a 6-month
duration. This was histopathologically reported as showing tuberculoid granulomatous infiltration that favored lupus vulgaris.
Slit-skin-smear was positive for Leishman-Donovan bodies and her diagnosis was cutaneous leishmaniasis. She was cleared with
intralesional sodium stibogluconate. Figure 15. A 25-year-old man presented with asymptomatic papules of 1-2 mm size on the face for a duration of 5-months. Histopathology was reported as tuberculoid granulomatous infiltration. These lesions responded to oral doxycycline and topical erythromycin; the condition cleared completely within 8 weeks. This was diagnosed lupus miliaris disseminatus faciei. | |
Although there are subtle histological features to differentiate these diseases depending on the spread of granulomata and lymphocytic response, definitive histological diagnosis can be difficult and inconclusive in cases in which specific features are absent, e.g., Leishman-Donovan bodies in leishmaniasis, copper pennies in chromomycosis. In these cases clinicopathological correlation is vital for diagnosis. Ancillary investigations such as PCR, culture, and QFT-2G can be considered depending on the availability.
The Mantoux test does not allow precise diagnosis, but only indicates that the patient has had previous contact with Mycobacterium tuberculosis; it can lead to false negative results in cases of anergy. Because of high rates of exposure to mycobacteria and BCG vaccination, the patients who had≥10mm diameter reactions were considered to have a positive Mantoux test in Sri Lanka. In our case series, although most of the patients showed inflammatory reactions to the Mantoux test, those that were <10mm diameter were considered negative. Seven of nine patients who had negative Mantoux tests were completely healed after CATI, whereas 1/5 patients who had positive Mantoux tests failed therapy.
Cultures for atypical mycobacteria cannot be performed in Sri Lanka. In some cases, one of which is the patient in Figure 12, differentiation between an atypical mycobacterial infection of soil origin or a granulomatous reaction to foreign particles was not determined.
Because PCR is expensive and was not freely available locally we did not perform this on the patients who responded poorly to CATI. Although PCR has emerged as the rapid, sensitive, and specific diagnostic method of pulmonary and extra-pulmonary TB, it has limited value in paucibacillary TB. When confirmed cases of paucibacillary TB were considered, the overall sensitivity was 73 percent. PCR positivity rates were 55 percent for tuberculosis verrucosa cutis (38 cases) and 60 percent for lupus vulgaris (5 cases) [9, 10].
In conclusion, if patients diagnosed with cutaneous TB do not respond significantly to CATI within 3 months, re-investigate for alternative diagnoses. This case series shows that for ESR, Mantoux reactivity, and TB cultures, although positive results facilitate clinical diagnosis, negative results do not exclude TB. These investigations showed high rates of false negative results in our case series. In the situation of limited investigative facilities, clinicohistopathological correlation with therapeutic response is the key to confirming cutaneous TB.
References
1. Asfar SF, Asfar I, Diniz G, Asilsoy S, Sorguc Y. Lupus vulgaris in a pediatric patient: A clinicohistopathological diagnosis. The Brazilian J Infectious Diseases 2008;12(2):152-154 [PubMed]2. Kratule RV, Apine RIA, Auzane MK. Problems of cutaneous tuberculosis. Probl Tuberk 1991;8:49-51 [PubMed]
3. Padmavathy L, lakshmana Rao L, Pari T, Ethirajan N, Krishnaswamy B. Lupus vulgaris and tuberculosis verrucosa cutis - a clinical, pathological and epidemiological study of 71 cases. Indian J Tuberc 2008;55(4):203-209 [PubMed]
4. Atukorala DN, Amerasekera LR. Tuberculosis of the skin in Sri Lanka. Ceylon Med J 1988 Sep;33(3):97-9. [PubMed]
5. Bukhari IA. Clinical patterns of cutaneous tuberculosis at King Fahad Hospital of the University in Al-Khobar, Saudi Arabia over 13 years. Saudi Med J 2009 Apr;30(4):577-8. [PubMed]
6. Akoglu G, Karaduman A, Boztepe G, Ozkaya O, Sahin S, Erkin G, Kolemen F. A case of lupus vulgaris successfully treated with antituberculous therapy despite negative PCR and culture. Dermatology 2005;211(3):189-190
7. Barbagallo J, Tager P, Ingleton R, Hirsch RJ, Weinberg JM. Cutaneous tuberculosis: diagnosis and treatment. Am J Clin Dermatol 2002;3(5):319-328 [PubMed]
8. Lodha R, Kabra SK. Newer diagnostic modalities for tuberculosis. Indian J Pediatr 2004;71:221-227 [PubMed]
9. Tan SH, Tan HH, Sun YJ, Goh CL. Clinical utility of PCR in the detection of Mycobacterium tuberculosis in different types of cutaneous tuberculosis and tuberculids. Ann Acad Med Singapore 2001;30(1):3-10 [PubMed]
10. Abdalla CM, de Oliveira ZN, Sotto MN, Leite KR, Canavez FC, de Carvalho CM. Polymerase chain reaction compared to other laboratory findings and to clinical evaluation in the diagnosis of cutaneous tuberculosis and atypical mycobacteria skin infection. Int J Dermatol 2009;48(1):27-35 [PubMed]
11. Hsiao PF, Tzen CY, Chen HC, Su HY. Polymerase chain reaction based detection of Mycobacterium tuberculosis in tissues showing granulomatous inflammation without demonstrable acid-fast bacilli. Int J Dermatol 2003 Apr;42(4):281-6 [PubMed]
12. Magana-Arachchi D, Perera J, Gamage S, Chandrasekharan V. Low cost in-house PCR for the routine diagnosis of extra-pulmonary tuberculosis. Int J Tuberc Lung Dis 2008 Mar;12(3):275-80 [PubMed]
13. Harada N. Characteristics of a diagnostic method for tuberculosis infection based on whole blood interferon-gamma assay. Kekkaku. 2006 Nov;81(11):681-6.
14. Orlando G, Merli S, Cordier L, Mazza F, Casazza G, Villa AM, Codecasa L, Negri E, Cargnel A, Ferrarese M, Rizzardini G. Interferon-gamma releasing assay versus tuberculin skin testing for latent tuberculosis infection in targeted screening programs for high risk immigrants. Infection. 2010 Jun;38(3):195-204. Epub 2010 Apr 22.
15. Kumar B, Rai R, Kaur I, Sahoo B, Muralidhar S, Radotra BD. Childhood cutaneous tuberculosis: a study over 25 years from northern India. Int J Dermatol 2001;40(1):26-32
16. Yasmeen N, Kanjee A. Cutaneous tuberculosis: a three year prospective study. J Pak Med Assoc. 2005 Jan;55(1):10-2 [PubMed]
17. Pandhi D, Reddy BS, Chowdhary S, Khurana N. Cutaneous tuberculosis in Indian children: the importance of screening for involvement of internal organs. J Eur Acad Dermatol Venereol 2004;18(5):546-551 [PubMed]
18. Bhutto AM, Solangi A, Khaskhely NM, Arakaki H, Nonaka S. Clinical and epidemiological observations of cutaneous tuberculosis in Larkana, Pakistan. Int J Dermatol 2002;41(3):159-65
© 2010 Dermatology Online Journal