Sweet syndrome
Published Web Location
https://doi.org/10.5070/D31zm2m110Main Content
Sweet syndrome
Edwin K Joe MD
Dermatology Online Journal 9(4): 28
From the Ronald O. Perelman Department of Dermatology, New York University
Abstract
Sweet syndrome is characterized by fever, leukocytosis, and tender, erythematous, well-demarcated papules and plaques, which show dense neutrophilic infiltrates and papillary dermal edema. It may occur in the absence of other diseases but is often associated with malignant conditions and may be induced by various medications. Treatment with systemic glucocorticoids generally is successful but may require prolonged courses to suppress recurrences.
Clinical Summary
History.—A 38-year-old woman presents with a 2-month history of an eruption involving the extremities, trunk, face, and neck. The patient first noticed a pruritic eruption on her legs. At that time, her primary-care doctor discontinued the patient's amlodipine, which had been started approximately 2 weeks earlier, and started metoprolol, benadryl, and hydrocortisone (1%) cream, without improvement. After 2 weeks, larger red lesions appeared on her arms that were occasionally pruritic, and fainter lesions on her upper back and face; the eruption on her legs began to resolve. She reports feeling feverish for 3 weeks prior to presentation. She also reports intermittent headaches over the last few years that have not changed recently. She denies recent sore throat, cough, rhinorrea, visual changes, joint aches, and vaccination. Her last menstrual period was 2 weeks prior to presentation.
Past medical history includes hypertension, stroke, iron-deficiency anemia, depression, and uterine fibroids status post myomectomies. Medications include metoprolol, aspirin, benadryl, citalopram, and iron.
Physical examination.—She has erythematous, edematous plaques, with surrounding erythema and less pronounced edema, involved her forearms; many had central ulcers. Broader, erythematous, slightly raised, edematous plaques are noted on her upper back, neck, and face. Hyperpigmented, slightly scaly papules and thin plaques are scattered on her lower legs.

|
|
| Figure 1 | Figure 2 |
|---|
Laboratory Data.—A complete blood count and differential analysis are normal except for a hematocrit of 35.8 percent. A comprehensive metabolic panel, including liver function tests, is normal. An erythrocyte sedimentation rate is 21 mm/hr, plasma C-reactive protein level is normal, glucose-6-phosphate dehydrogenase level is 6.4 U/g Hb. A chest radiograph is ordered. A recent noncontrast head computed tomography shows a slightly enlarged right globe without any visualized orbital lesions.
A punch biopsy was performed on her left arm. The patient is started on oral cephalexin, hydroxyzine, topical triamcinolone acetonide (0.1 %) ointment, and hydrocortisone (2.5 %) cream.
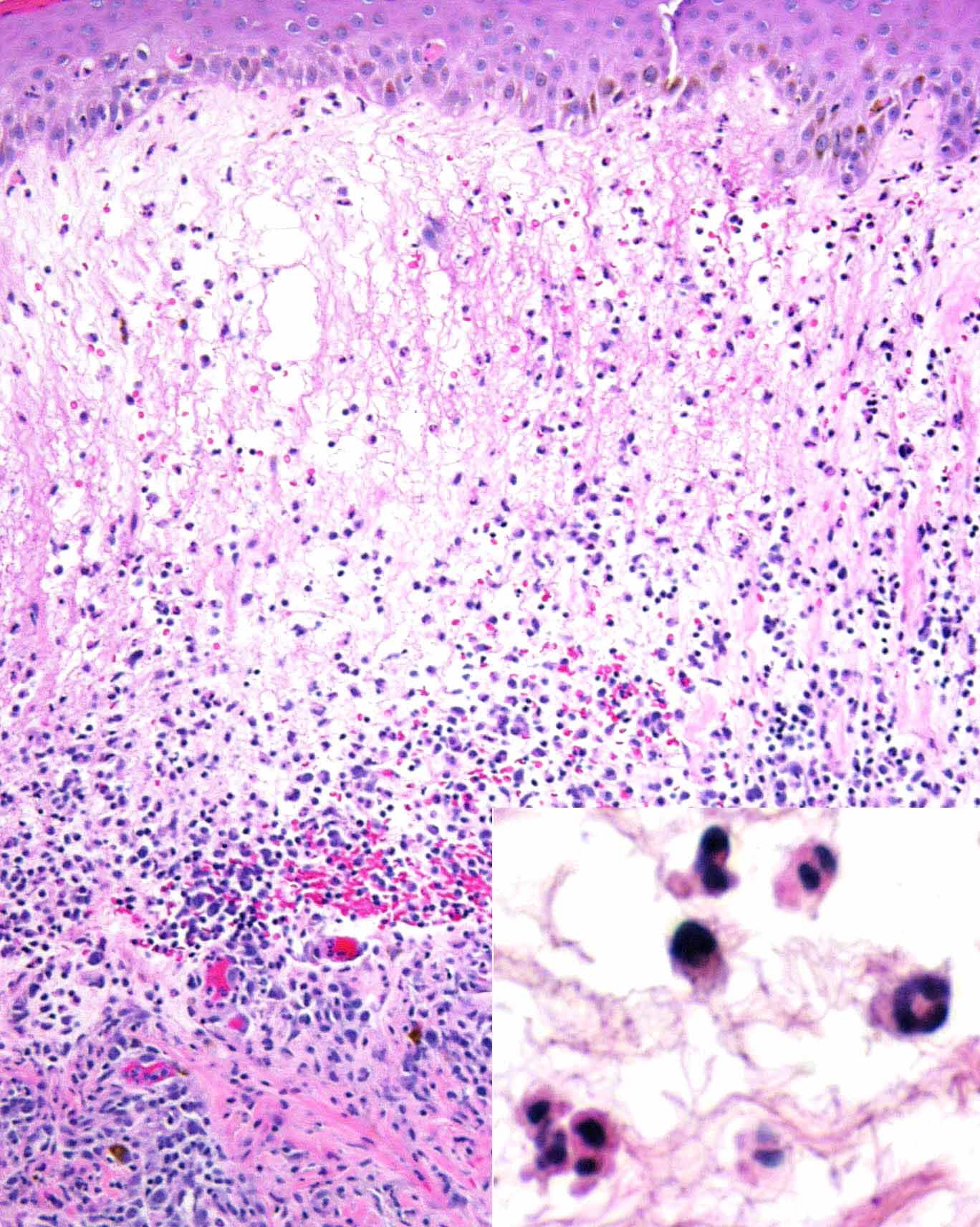
Histopathology.—Hematoxylin-and-eosin stained sections show a superficial and deep perivascular and interstitial infiltrate of numerous neutrophils, with scattered lymphocytes and plasma cells. There is marked papillary dermal edema, many extravasated erythrocytes, and focal spongiosis of the overlying epidermis. No vasculitic changes are noted.
Diagnosis.—Acute febrile neutrophilic dermatosis (Sweet syndrome).
Comment.—Acute febrile neutrophilic dermatosis was first described by Sweet in 1964. There is a broad incidence peak in the fourth to seventh decades; women average age 50 and men age 65. Disease onset clusters in the spring and autumn. The etiology is unknown but is thought to be a hypersensitivity reaction that leads to cytokine stimulation and subsequent neutrophil activation and infiltration [1]. Sweet syndrome presents in three clinical settings: a classic or idiopathic form; a malignancy-associated or paraneoplastic form; and a drug-induced form [1]. Associated malignant conditions are usually hematologic, most commonly acute myelogenous leukemia. Carcinomas of the breast and of the genitourinary and gastrointestinal tracts are the most frequently reported solid tumors [2]. Medications implicated in drug-induced Sweet syndrome include granulocyte-colony stimulating factor, minocycline, trimethoprim-sulfamethoxazole, antiepileptics, antihypertensives, oral contraceptives, or retinoids [1]. The clinical features of Sweet syndrome are summarized below [1]:
| Table 1. Sweet Syndrome (% occurrence) | ||||
| Characteristic | Classical | Hematologic | Solid tumor | Drug-induced |
| Epidemiology: | ||||
| Women | 80 | 50 | 59 | 71 |
| Prior upper respiratory tract infection | 75-90 | 16 | 20 | 21 |
| Recurrence | 30 | 69 | 41 | 6 7 |
| Clinical symptoms: | ||||
| Fever | 80-90 | 88 | 79 | 100 |
| Musculoskeletal involvement | 12-56 | 26 | 34 | 21 |
| Ocular involvement | 17-72 | 7 | 15 | 21 |
| Lesion location: | ||||
| Upper extremities | 80 | 89 | 97 | 71 |
| Head and neck | 50 | 63 | 52 | 43 |
| Trunk and back | 30 | 42 | 33 | 50 |
| Lower extremities | Infrequent | 49 | 48 | 36 |
| Oral mucous membranes | 2 | 12 | 3 | 7 |
| Laboratory findings: | ||||
| Neutrophilia | 80 | 47 | 60 | 38 |
| Elevated erythrocyte sedimentation rate | 90 | 100 | 95 | 100 |
| Anemia | Infrequent | 82 | 83 | 100 |
| Abnormal platelet count | Infrequent | 68 | 50 | 50 |
| Abnormal renal function | 11-50 | 15 | 7 | 0 |
Cutaneous lesions are characterized by tender, erythematous plaques; occasionally, pustules, bullae, or ulcers develop. Burning, but not pruritus, typically is reported. Involvement of the eyes, joints, lung, liver, kidney, heart, and pancreas have been described [3]. Diseases associated with Sweet syndrome include inflammatory bowel disease, and infections of the upper respiratory tract (e.g., streptococcosis) and the gastrointestinal tract (e.g., yersiniosis). Pregnancy and vaccination are associated in 2 percent [1].
The differential diagnosis for Sweet syndrome includes bowel bypass-related dermatosis, cellulitis or erysipelas, erythema nodosum, erythema multiforme, urticaria, necrotizing vasculitis, erythema elevatum diutinum, and pyoderma gangrenosum [1].
The diagnostic criteria are summarized below [1]:
Criteria Classic / Malignancy-associated Drug-induced 1 Abrupt onset of painful erythematous plaques/nodules 2 Histopathologic evidence of a dense neutrophilic infiltrate without evidence of leukocytoclastic vasculitis. 3 Fever > 38° C 4 Association: underlying malignancy, inflammatory disease, pregnancy; OR preceded by upper respiratory or gastrointestinal infection or vaccination. Temporal relationship: between drug ingestion and clinical presentation; OR recurrence after oral challenge 5 Excellent response to treatment with systemic glucocorticoids or potassium iodide. Temporally related resolution of lesions after drug withdrawal or treatment with systemic glucocorticoids. 6 Abnormal labs at presentation (3 of 4): ESR > 20mm/hr, (+) C reactive protein, WBC > 8000, neutrophils > 70 percent Diagnosis Both major criteria (1 and 2), and 2 of 4 minor criteria (3-6). All 5 criteriaThe most prominent histologic findings include a dense infiltrate of neutrophils in the superficial dermis and papillary dermal edema. Mononuclear cells and occasional eosinophils may be present. Additional findings may include leukocytoclasis and vesicles or bullae [1].Sweet syndrome responds rapidly to systemic glucocorticoids. Prolonged treatment may be needed to suppress recurrences, which are common. Localized lesions may be successfully treated with intralesional or topical glucocorticoids. Alternative treatments include doxycycline, potassium iodide, colchicine, indomethacin, dapsone, cyclosporine, cyclophosphamide, chlorambucil, and clofazamine [1].
References
1. Cohen PR, et. al. Sweet's syndrome: A neutrophilic dermatosis classically associated with acute onset and fever. Clin Dermatol. 2000; 18:265.2. Hensley CD, et. al. Neutrophilic dermatoses associated with hematologic disorders. Clin Dermatol. 2000; 18:355.
3. Vignon-Pennamen MD. The extracutaneous involvement in the neutrophilic dermatoses. Clin Dermatol. 2000; 18:339.
© 2003 Dermatology Online Journal