Familial yellow nail syndrome
Published Web Location
https://doi.org/10.5070/D31sp2v29kMain Content
Familial yellow nail syndrome
Ebrahim Razi MD
Dermatology Online Journal 12 (2): 15
Section of Internal Medicine, Kashan University of Medical Sciences, Kashan, Iran. ebrahimrazi@yahoo.comAbstract
A 70-year-old woman with yellow nail syndrome and right-sided pleural effusion, lower extremity edema, and hypoalbuminemia was followed for 18 months. She reported an 8-year history of asthma. She had four children (3 boys and 1 girl). Dystrophy, changes in color and shape of nails both hands and foot, along with lower extremity edema was observed in the daughter and two of her sons. One son had asthma. The patient reported that her grandmother had similar nail abnormality and lower extremity edema. Other family members and patient's grandchildren were healthy. This report demonstrates a case of familial yellow-nail syndrome.
Introduction
The yellow nail syndrome (YNS), first described in 1964 by Samman and White[1], is characterized by the presence of dystrophic, thickened, and slow-growing yellow nails in association with peripheral edema. It is a rare condition with fewer than 100 reported cases.
The manifestations of YNS have been extended to include pleural effusion [2, 3], bronchial hyperresponsiveness [4], bronchiectasis [5], chronic bronchitis, chronic sinusitis, and lymphedema (most frequently of the lower extremity). Most cases reported are idiopathic, however the syndrome has been described in association with malignancy [6]. Familial occurrence of YNS also has been reported (5).
We present a patient with familial YNS associated with pulmonary findings, lymphedema, and hypoproteinemia in a 70-year-old woman; manifestations of this syndrome were also present in her three siblings.
Case report
A 70-year-old woman was admitted for evaluation of a right-sided pleural effusion. She had a history of dyspnea and asthma for 8 years and was treated with an anti-asthmatic drug. On examination her temperature was 36.5°C, blood pressure 120/70 mm, respiratory rate 28 breaths/minute, and pulse 93 beats/minute. Examination of the chest revealed dullness on percussion, with decreased breath sounds in the lower half of the right lung, bilateral expiratory wheezing, and pitting edema of the legs. All 20 nails showed a yellowish discoloration with thickening of the nail plates and disappearance of the cuticles (Fig. 1). Nail growth was almost totally arrested.
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Yellowish discoloration, thickening of the nail plate, and disappearance of the cuticle on both hands and feet in the 70-year-old patient. | |
| Figure 2. Her chest x-ray reveals right-sided pleural effusion. | |
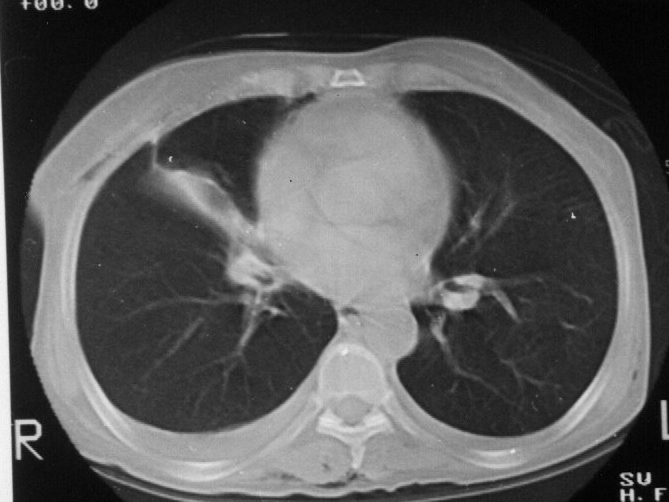
Laboratory studies showed the following: WBC of 15,600/ml (80 % neutrophils, 18 % lymphocytes, 2 % monocytes); a hemoglobin level of 15.2 g/dl, and a platelet count of 380,000/ml. The total protein level was 5.5 g/dl (normal: 6.4 to 8.4 g/dl); asparate aminotransferase, 35 U/L (normal: 0 to 33 U/L); alanine aminotransferase and alkaline phosphatase was normal. The erythrocyte sedimentation rate was 3 mm/hour. Urinalysis showed a pH of 8, negative for albumin, and no cells. Chest X-ray showed a right sided pleural effusion (Fig. 2). A thoracentesis yielded yellow fluid; with a lactate dehydrogenase level of 315 U/L (normal 100-500 U/L); protein content was 2.2 g/dl; glucose content was 79 mg/dl; pleural fluid total cell was 3780/ml (white blood cell 3680/ml with neutrophils 94 % and lymphocytes 6 %). Concomitant serum lactate dehydrogenase was 341 U/dl. Cytologic examination did not reveal malignant cells, and the results of acid fast bacillus study and culture were negative. The PPD test was negative. Arterial blood gas value on room air revealed a pH of 7.36, a carbon dioxide partial pressure of 47.6 mm Hg, and oxygen partial pressure of 64.1 mm Hg and HCO3 26.4 mmol/l. Computed tomographic (CT) scan of the chest demonstrated bronchiectasis and fibrotic changes in anterior segment of the right upper lobe (Fig. 3).
 |
| Figure 3 |
|---|
| CT scan revealing bronchiectasis and fibrotic changes in anterior segment of the right upper lobe and right-sided pleural effusion. |
After 18-months followup the patient was hospitalized again, this time with bilateral pleural effusions, worsening of lower extremity edema, and ascites. Treatment with furosemide, intravenous albumin, and low-salt regimen was begun. The pedal edema subsided and the patient was discharged. After 3 months her condition deteriorated, and the patient was readmitted because of exacerbation of ascites, extremity edema, and progressive bilateral pleural effusions. Despite treatment for respiratory failure with mechanical ventilation and aspiration of large pleural fluids, the patient died of nosocomial pneumonia and a complication of mechanical ventilation.
The patient had four children (3 boys and 1 girl). She was related to her husband before the marriage (the husband was the son of paternal aunt and she was the daughter of a paternal uncle). The 36-year-old daughter and 33- and 40-year old sons had manifestations of this syndrome. They were noted to have changes in color and shape of fingernails and toenails (Figs. 4-6). The 33-year-old son also had asthma. The patient reported similar nail abnormalities and lower extremity edema in her grandmother. Other family members and the patient's grandchildren were healthy.
 |  |
| Figure 4 | Figure 5 |
|---|---|
| Figure 4. Yellow fingernails of the 36-year-old daughter. The nail is dystrophic and the nail growth is arrested. | |
| Figure 5. Toenails of the 33 year-old son who also has lymphedema and asthma. | |
 |  |
| Figure 6a | Figure 6b |
|---|---|
| Dystrophic toenails of the 40 year-old son who also has lower extremity edema. | |
Comments
It appear that familial YNS is present in grandmother and three children of patient. Two siblings have been described who manifested signs of both the syndrome and immunologic deficiency; however, this familial occurrence is unique among the case reported to date [5].
The syndrome of yellow nails and lymphedema was first described by Samman and White in 1964 [1]. Later, Emerson[2] added pleural effusion as a frequent feature of the disease. The diagnosis is based on the characteristic triad of yellow nails, lymphedema, and respiratory involvement. However, these three alterations are simultaneously present in only 27 percent of cases [7]. In 1986 Nordkild and associates reviewed the reports of the 97 patients described in the literature [6]. The median age at onset was 40 years, however, the age of onset varies widely; for example, lymphedema may be present at birth or become manifest at the age 65. Yellow nails were present in 89 percent of the patients, 80 percent had lymphedema of varying severity, and 36 percent had pleural effusion. In 29 percent of patients, the initial symptom was related to pleural effusion.
Patients often give a history of recurrent attacks of bronchitis and may have chronic sinusitis, bronchiectasis, and recurrent pneumonia. Of the twelve patients reported from the Mayo Clinic, eight had recurrent pleural effusion and five had bronchiectasis; in this series, the first manifestation of the syndrome was either lymphedema or yellow nails, pleural effusion appearing somewhat later in all cases. The pleural effusion is usually exudative, either idiopathic or secondary to infection or chylothorax. The pleural fluid characteristically contains a high percentage of lymphocytes [8].
The pathogenesis of the bronchiectasis is unknown, although it is frequently associated with sinusitis; in one patient the bronchiectasis was confined to the upper lobes [9]. The YNS has been reported in association with thyroid disease [6], hypogammaglobulinemia [6], nephrotic syndrome [6], protein-losing enteropathy [10], obstructive sleep apnea [11], and xanthogranulomatous pyelonephritis [12].
Many nail alterations have been described in association with YNS as follows: thickening, hardening, longitudinal over-curvature, total or distal yellow discoloration, loss of cuticle, transverse ridging associated with variations in the ungual growth rate, and onycholysis that may lead to shedding. Erythema and edema of the proximal nail fold or chronic paronychia also may be present [7]. The nail growth is slow (0.1-0.25 mm/week, normal 0.5-2 mm/week) [13]. Dermatophytic superinfection had been reported rarely [14].
The pathogenesis of nail abnormalities remains unknown. Lymphatic vessel alterations may play a role in some cases. DeCoste et al. hypothesized that primary sclerosis of the stroma could lead to lymphatic obstruction [15]. The slower ungual growth may be a result of slow lymphatic flow. In 7-30 percent of cases, there is a spontaneous partial or total remission [1, 16]. But relapse often occurs. Nail improvement is often concomitant with improvement of the respiratory pathology [4, 15]. Defective lymph drainage and lymphedema is attributed to hypoplasia (sometimes atresia) of the lymphatics, defects that can be demonstrated by peripheral lymphangiography. Impaired lymphatic function has been considered an underlying abnormality in YNS, and perhaps even the primary problem. In YNS, edema results from and imbalance between capillary filtration and lymph flow.
Lymphedema, by definition, is edema due to a reduction in lymph flow. Many chronic edema are of mixed etiology, i.e., attributed to impaired lymph flow in the face of raised filtration rate. The reversibility of the edema suggests that any lymphatic insufficiency is functional and not structural. The widespread nature of fluid accumulation in YNS, including peripheral edema, pleural effusions and ascites, also suggest a functional rather than an anatomic disorder. There is no evidence to suggest that other factors influencing edema, such as salt or water imbalance, or hapoproteinemia, play a part in the genesis of YNS. Although lymphedema may be associated with YNS, the reversible nature of the edema excludes a primary structural abnormality in YNS and suggest that lymphatic involvement is secondary, and probably functional, in nature [17].
An inflammatory component, which could alter both blood flow and capillary permeability has not been excluded in the pathogenesis of the edema in the YNS. Interestingly, topical vitamin E, which has been used to treat nail in YNS, has and anti-inflammatory action [13, 16].
In summary, this report shows a case of familial YNS with implications of genetic factors in the pathogenesis of the disease. On the basis of this observation, it appears essential that family history be considered in the characterization of the disease.
References
1. Samman PD, White WF. The 'Yellow nail' syndrome. Br J Dermatol. 1964 Apr;76:153-7. PubMed2. Emerson PA. Yellow nails, lymphoedema, and pleural effusions. Thorax. 1966 May;21(3):247-53. PubMed
3. Dilley JJ, kierland RR, Randall RV, Shick RM. Primary lymphedema associated with yellow nails and pleural effusions. JAMA. 1968 May 20;204(8):670-3. PubMed
4. Luyten C, Andre J, Walraevens C, De Doncker P. Yellow nail syndrome and onychomycosis. Experience with itraconazole pulse therapy combined with vitamin E. Dermatology. 1996;192(4):406-8. PubMed
5. Hiller E, Rosenow EC, Olsen AM. Pulmonary manifestations of the yellow nail syndrome. Chest. 1972 May;61(5):452-8. PubMed
6. Nordkild P, Kromann - Andersen H, Struve - Chirstensen E. Yellow nail syndrome--the triad of yellow nails, lymphedema and pleural effusions. A review of the literature and a case report. Acta Med Scand. 1986;219(2):221-7. PubMed
7. Tosti A, Baran R, Dawber RPR: The nail in systemic diseases and drug - induced changes: in Baran R, Dawber RPR (eds): Diseases of the Nails and Their Managements, ed 2. Oxford, Blackwell, 1994, PP 175-261.
8. Solal - Celigny P, Cormier Y, Fournier M. The yellow nail syndrome .Llight and electron microscopic aspects of the pleura. Arch pathol Lab Med 1983; 107: 183-85. PubMed
9. McNicholas WT, Quigley C, FitzGerald MX: Upper lobe bronchiectasis in the yellow nail syndrome: report of a case. Ir J Med Sci. 1984 Nov;153(11):394-5. PubMed
10. Battaglia A, Di Ricco G, Mariani G, Giuntini C. Pleural effusion and recurrent broncho-pneumonia with lymphedema, yellow nails and protein-losing enteropathy. Eur J Respir Dis. 1985 Jan;66(1):65-9. PubMed
11. Knuckles ML, Hodge SJ, Roy TM, Snider HL. Yellow nail syndrome in association with sleep apnea. Int J Dermatol. 1986 Nov;25(9):588-9PubMed
12. Danenberg HD, Eliashar R, Flusser G, Rosenmann E, Chajek-Shault. Yellow nail syndrome and xanthogranulomatous pyelonephritis. Postgrad Med J. 1995 Feb;71(832):110-1. PubMed
13. Williams HC, Buffham R, du Vivier A. Successful use of topical vitamin E solution in the treatment of nail changes in yellow nail syndrome. Arch Dermatol. 1991 Jul;127(7):1023-8. PubMed
14. Venencie PY, Dicken CH. Yellow nail syndrome: report of five cases. J Am Acad Dermatol. 1984 Feb;10(2 Pt 1):187-92. PubMed
15. DeCoste SD, Imber MJ, Baden HP. Yellow nail syndrome. J Am Acad Dermatol. 1990 Apr;22(4):608-11. PubMed
16. Norton L. Further observation on the yellow nail syndrome with therapeutic effects of oral alpha - tocopherol. Cutis 1985 Dec; 36(6): 457-62. PubMed
17. Bull RH, Fenton DA, Mortimer PS. Lymphatic function in the yellow nail syndrome. Br J Dermatol. 1996 Feb;134(2):307-12. PubMed
© 2006 Dermatology Online Journal