Merkel cell carcinoma: Treatment with bleomycin
Published Web Location
https://doi.org/10.5070/D315r9n6k0Main Content
Merkel cell carcinoma: Treatment with bleomycin
Haines Ely MD1, Annabella Pascucci2
Dermatology Online Journal 14 (9): 3
1. Department of Dermatology, University of California Davis, Sacramento, California2. School of Medicine, UC Davis, Sacramento, California
Abstract
Merkel cell carcinoma is the second most deadly form of skin cancer after melanoma, with a mortality rate of as high as 35 percent. It usually occurs as a deep red or purple dome-shaped tumor on sun-exposed skin of elderly people. Transplant recipients or AIDS patients have a higher incidence of this tumor than normal individuals. There is an association of a polyoma virus with this tumor that may explain the increased incidence in immunosuppression. Surgery, followed by radiation therapy is the standard of treatment. Sentinel node dissection is recommended because this tumor metastasizes often. Chemotherapy, such as is used for oat cell carcinoma of the lung, is advised for metastatic disease. However, systemic chemotherapy protocols have not been overly successful. We have treated four cases of stage-I Merkel cell carcinoma with surgery followed by intralesional bleomycin and have followed these cases for up to five years with no evidence of recurrence or metastasis. One case had radiation post operatively but the tumor recurred. Intralesional bleomycin caused complete regression of this tumor with minimal scarring and long term cure. Bleomycin, besides being a potent chemotherapy agent, has direct antiviral effects that may explain why this drug is so effective in treating Merkel cell carcinoma.
Merkel cell carcinoma (MCC) is a rare and aggressive cutaneous cancer first described by Toker in 1972 as a trabecular carcinoma of the skin [1]. Since that time, hundreds of papers have been published on the topic. An excellent web site has been set up by Paul Nghiem MD that constantly updates new information on this tumor. Merkel cell carcinoma has an incidence of 0.24 per 100,000 person-years and affects a disproportionate number of white elderly people. It is estimated that 76 percent of those affected are older than 65 years and 94 percent are light skinned. Males have an incidence of 1.5-2:1 in all ethnic groups compared to females. The incidence of MCC has been increasing over time, which could be secondary to improved detection or an aging population [2]. A major risk factor for development of MCC is sun exposure, and there is a correlation between UVB index and incidence of MCC. There is also a reported 100-fold increase in the incidence of MCC in patients with psoriasis treated with PUVA [3]. Feng et al. have shown the association of a polyoma virus with this tumor [4]; this may explain the increased incidence in immunosuppression. Immunocompromise and immunosuppression seems to play a role, because MCC has a higher incidence in transplant patients and those affected by human immunodeficiency virus (HIV). Engels et al. found the relative risk of MCC in HIV positive patients to be 13.4 as compared with the general population [5]. Transplant patients are affected at a younger age, with 29 percent being less than 50 years old compared to only 5 percent of the general population [6].
Merkel cell carcinoma typically presents as a painless, rapidly growing, dome-shaped, red nodule on a sun-exposed area. It is often initially misdiagnosed. Heath et al. have recently proposed the acronym AEIOU to describe the most common clinical characteristics: asymptomatic, expanding rapidly, immune suppression, older than 50 years, UV-exposed site on fair skin [7]. Histological confirmation shows aggregates of small round blue cells present in the dermis and often extending into subcutaneous fat. The cells have hyper-chromatic nuclei, scant cytoplasm, and frequently have mitoses present. Histopathologic findings are similar to other small cell tumors, making immunohistochemistry necessary to confirm the diagnosis. The CK-20 marker is sensitive for MCC and stains in a paranuclear dot pattern. Merkel cell carcinoma is negative for S100, CK-7, and common leukocyte antigen; this distinguishes it from melanoma, bronchial small cell carcinoma, and cutaneous lymphoma, respectively [8]. McKee states that CK-20 is positive in 90 percent of cases and neuron-specific enolase (NSE) is positive 80 percent of the time [9]. The CK-20 antigen is useful if one suspects a small cell tumor metastatic to the skin from an unknown lung primary (a very unlikely scenario). We feel a chest X ray is a more cost effective way of ruling out lung cancer.
In our cases neuron-specific enolase is almost always positive and this is the first special stain ordered if there is any difficulty distinguishing MCC from basal cell carcinoma (BCC) [10]. Merkel cell carcinoma may be misdiagnosed as BCC both clinically and histologically [11]. The CK-17 antigen is positive in basal cell carcinoma and negative in MCC [11].
Staging of MCC has been done using a three or four tiered staging system. The four-tiered staging system takes tumor diameter into account, because it has been found to be an independent predictor of survival. Using the four tiered system, stage I is a primary tumor with diameter <2cm, stage II is a tumor with diameter >2cm, stage III has lymph node metastasis, and stage IV has distant metastatic disease [3]. Sentinel lymph node biopsy (SLNB) should be a part of the staging system. SLNB detects lymph node involvement in patients who would otherwise be clinically or radiologically understaged. It also plays an important role in treatment, because adjuvant nodal therapy provides a benefit in SLNB positive patients [12].
There are no clear treatment guidelines for MCC, and the treatment modalities used depend on MCC stage. Surgery is clearly the initial treatment for localized disease, but there is no consensus on the recommended size of local excision. There are proponents for wide local excision of at least 2cm margins, some for 1cm, and some for the use of Mohs microsurgery [3]. The small blue cells are easily seen during Mohs procedures. There is also difference of opinion regarding the use of adjuvant radiotherapy (RT) after excision of primary MCC. Lewis et al. found lower rates of local and regional recurrence in patients treated with adjuvant RT compared with those treated with surgery alone, although survival is less clearly affected [13]. Patients with SLNB positive status must undergo either complete lymph node dissection (CLND) or adjuvant nodal RT. Complete lymph node dissection is currently considered the first line treatment for micrometastasis, but nodal RT has been used with success when there is a high morbidity associated with CLND [4, 8]. Radiotherapy has also been used as monotherapy in patients with inoperable disease because of age or location, and was found to produce similar outcomes to conventional therapy of surgery with adjuvant RT [14]. There is even less consensus regarding the use of chemotherapy (CT) and it is the least studied form of therapy. It also has a high morbidity associated with it and for that reason tends to be used mostly in patients with stage-IV disease. The most common systemic CT drugs used have been carboplatin, etoposide, cisplatin, doxorubicin, and vincristine. Merkel cell carcinoma is a radiosensitive tumor and appears to respond well to these drugs, but CT treatment has yet to show a survival benefit [3].
We report four cases of stage I MCC treated with intralesional bleomycin followed for up to 5 years with no evidence of recurrence or metastasis.
Clinical synopses
Case 1
 |  |
| Figure 1a | Figure 1b |
|---|---|
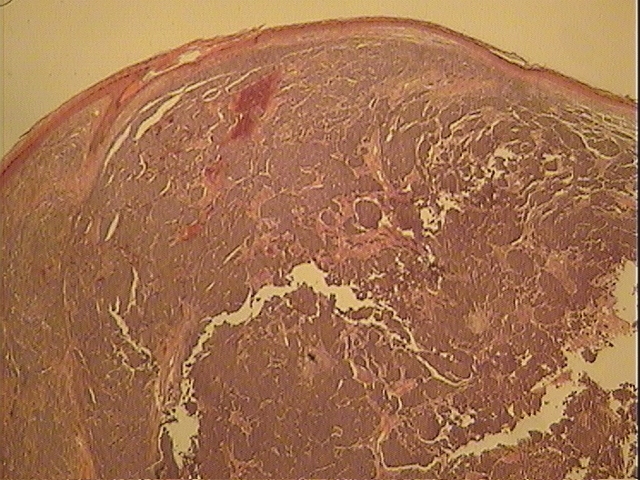
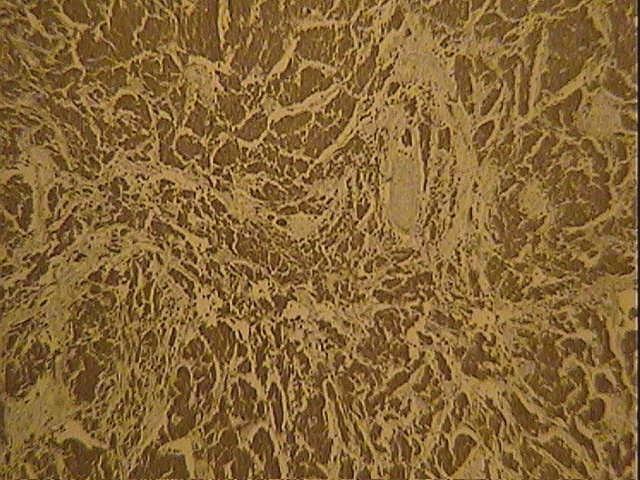
| Figure 1a. MCC of right forearm Figure 1b. Histology (hematoxylin & eosin) | |
 |  |
| Figure 1c | Figure 2a |
|---|---|
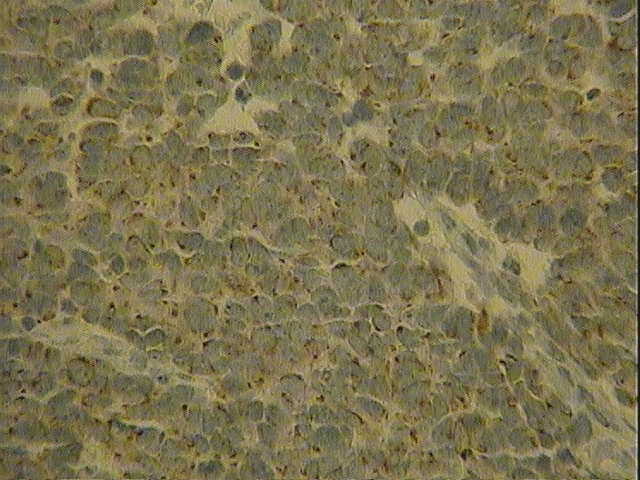
| Figure 1c. CK-20 stain Figure 2a. Reaction to bleomycin one week after initial injection | |
 |  |
| Figure 2b | Figure 3 |
|---|---|
| Figure 2b. Reaction to bleomycin after second injection Figure 3. Patient's forearm showing no evidence of local recurrence | |
An 85-year-old woman presented in October 2005 with a dome-shaped, deep red tumor on her right forearm, measuring 1.4 cm in diameter (Fig. 1a). The tumor was excised for biopsy and histology results confirmed a diagnosis of MCC (Figs. 1b, 1c). The patient decided to defer surgery until after attending a wedding, and later refused surgery altogether. She instead opted for local chemotherapy. In November 2005, five international units (IU) of bleomycin were injected into the scar of the biopsy site. The patient reported chills two hours after receiving the shot. On exam, there were no palpable lymph nodes. Labs were within normal limits and chest x-ray was negative. On follow-up two weeks after the initial injection, the tumor site was pink, flat, and without ulceration (Fig. 2a). The patient received a second intralesional injection of bleomycin in November 2005, again at a dose of five IU. In follow-up two weeks after the second shot, the lesion was again pink and flat, this time with associated itching (Fig. 2b). The site was re-excised for biopsy in April 2005. There was no evidence of tumor either on H&E stain or neuron-specific enolase stained sections. Patient remains cured as of April 2008 (Fig. 3).
Case 2
 |  |
| Figure 4 | Figure 5 |
|---|---|
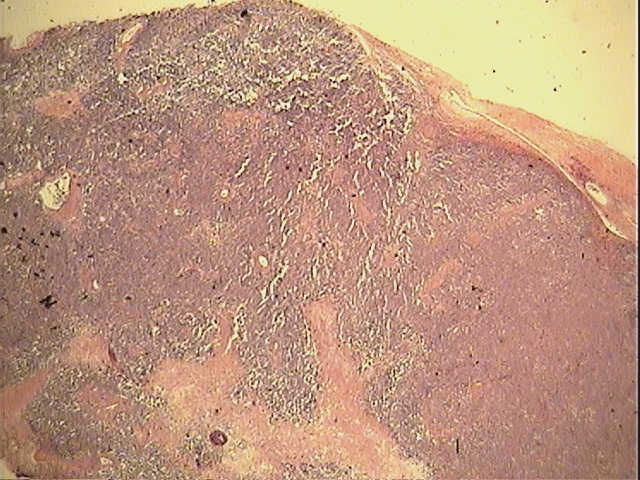
| Figure 4. MCC pre radiation therapy, Case 2 Figure 5. Merkel cell carcinoma, recurrent after radiation therapy | |
 |  |
| Figure 6 | Figure 7 |
|---|---|
| Figure 6. Merkel cell carcinoma after first injection of blomycin Figure 7. Merkel cell carcinoma after second injection of bleomycin | |
 |
| Figure 8 |
|---|
| Figure 8. Merkel cell carcinoma one year after bleomycin therapy |
An 84-year-old woman presented with a rapidly growing tumor of the right zygoma, measuring 6cm in diameter. Biopsy was done and results showed MCC (Fig. 4). The local surgeons refused to remove tumor and the patient underwent radiation therapy instead. She initially received 1000cGy of radiation in a single fraction on July 25, 2001. On August 24, 2001 the tumor was 1.3 cm in size, and 1000cGy of radiation was again given in single fraction using 12 MeV electrons. In November 2001 there was a huge tumor re-growth (Fig. 5). On December 13, 2001, five IU of bleomycin was injected directly into tumor base (Fig. 6). One week later, five IU of bleomycin was again injected intralesionally into the now barely visible tumor (Fig. 7). The patient had no evidence of recurrence five years after the original diagnosis of MCC (Fig. 8). This case was presented in 2002 at the Pacific Dermatologic Association annual meeting CPC and was discussed by A. Bernard Ackerman MD.
Case 3
 |  |
| Figure 9 | Figure 10 |
|---|---|
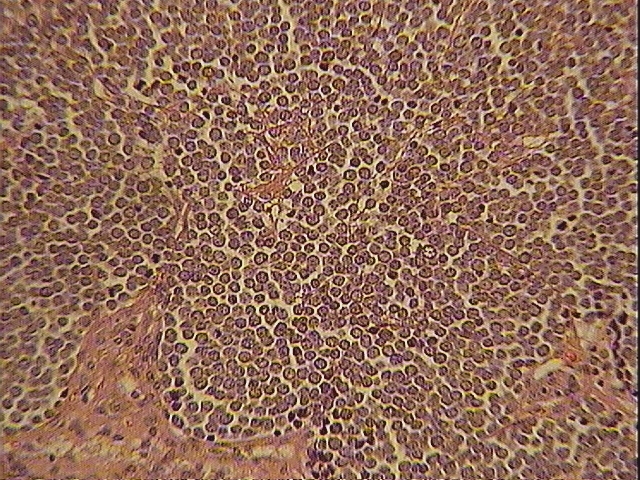
| Figure 9. Merkel cell carcinoma of ear Figure 10. Case 3: Merkel cell carcinoma of ear | |
 |  |
| Figure 11 | Figure 12 |
|---|---|
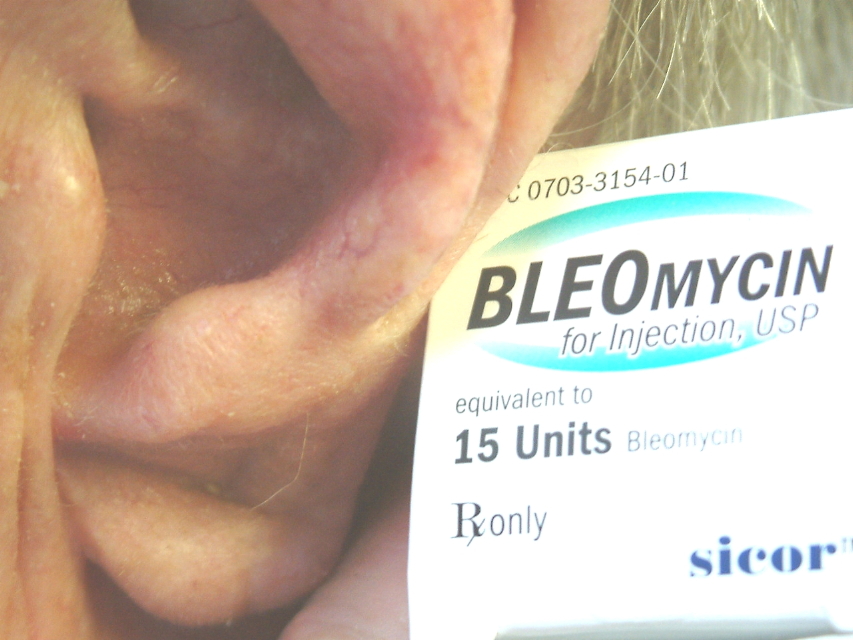
| Figure 11. Positive NSE stain, case 3 Figure 12. Case 3: The original tumor was adjacent to the letter "B" in bleomycin. No evidence of recurrence as of April 2008 | |
A 63-year-old man presented on June 6, 2006, with a tumor on left ear antehelix (No tumor photo, but it was very similar to Figure 9). Biopsy was obtained and showed MCC (Figs. 10, 11). The patient received five intralesional injections consisting of five IU of bleomycin between June 26 and July 24, 2006; by the end of treatment the patient appeared cured. Tumor site was re-biopsied on August 15, 2006, and results showed no evidence of tumor, with a negative NSE stain. The patient continues to have no recurrence as of April 2008 (Fig. 12).
Case 4
 |  |
| Figure 13 | Figure 14 |
|---|---|
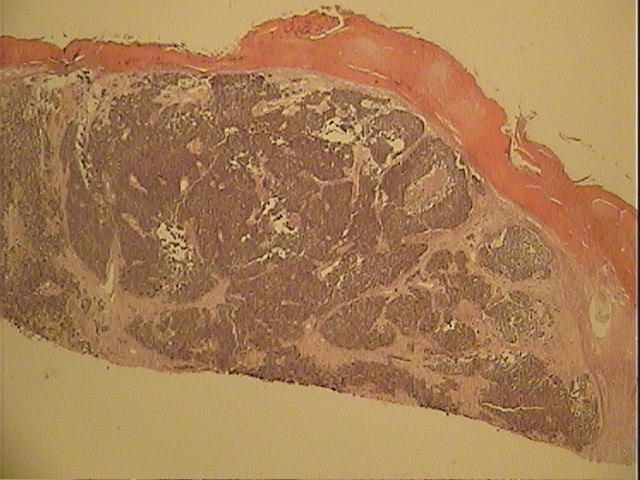
| Figure 13: Case 4 Figure 14. Case 4 Histopathology of MCC (H&E) | |
 |
| Figure 15 |
|---|
| Figure 15: Positive NSE stain case 4 |
An 80-year-old man presented with plum-colored tumors on his right cheek (Fig. 13). They were biopsied on October 22, 1990, and were found to be MCC (Figs. 13, 14, 15). The tumors were widely excised with a 3cm border on October 31 1990. Sutures were removed one week later, and wound edges were injected with five IU of bleomycin. The wound edges were again injected with five IU of bleomycin on November 20, 1990. The patient met with a radiation oncologist the next day and refused therapy. However, the patient's oncologist and family convinced him to undergo radiation treatment even though he was asymptomatic and had no palpable neck nodes. In April 1991, he was treated with 6000 cGy to the surgical area and 5000 cGy to neck nodes. He suffered with dryness, pain, and red skin for months following radiation treatment. The patient was diabetic. He died several years later from sepsis secondary to osteomyelitis.
Discussion
Merkel cell carcinoma is a rare and aggressive tumor that has been treated with surgery, radiation, chemotherapy, or a combination of all three. There are no treatment guidelines for MCC and no consensus regarding when to use radiotherapy or chemotherapy. In this paper, we report four cases of stage I MCC treated with intralesional bleomycin followed for up to five years with no evidence of recurrence or metastasis.
Bleomycin is an antibiotic isolated from cultures of Streptomyces verticillus that was found to have anti-neoplastic effects. It binds and degrades double-stranded DNA in a sequence-specific manner and has more recently been shown to cleave RNA as well [15]. Bleomycin interacts with DNA at 5'-GT-3' and 5'-GC-3' sequences, but its interaction with RNA seems to be mostly related to RNA tertiary structure instead of the primary sequence [15]. The interaction with tertiary structure suggests that bleomycin might be able to act selectively against oncogenic RNA viruses [15]. Bleomycin has been shown to have antiviral effects against the hepatitis C virus [16] and a European use patent suggests it is effective against HIV virus [17].
Feng et al. discovered that MCC is caused by previously unknown polyoma virus [4]. The virus is a small DNA virus, icosahedral in shape, with no lipoprotein envelope. Human pathogens in this virus group include BK virus, JC virus, and Merkel cell carcinoma virus. Polyoma virus used to be one of two genera within the now obsolete papovaviridae family, the other genus being Papillomavirus [4]. Human papovavirus is extremely susceptible to bleomycin. Since 1970 when it was first used for warts millions of patients have been cured by intralesional bleomycin therapy.
Intradermal injections of bleomycin into normal human skin have been postulated to cause direct or indirect cytotoxicity to keratinocytes and eccrine epithelium. There appears to be a cellular immune response and pro-inflammatory cytokine secretion at these sites [18]. How this translates to its effectiveness against certain skin lesions is uncertain. Bleomycin previously has been used with success in the treatment of warts, keratoacanthomas, keloids, hemangiomas, lesions of Kaposi sarcoma, early squamous cell carcinoma, and basal cell carcinoma [19]. We are the first to describe the use of intralesional bleomycin for the treatment of stage I Merkel cell carcinoma.
The most convincing proof to us that bleomycin is an effective treatment of MCC is the effect seen on patient 2. This patient's tumor recurred after radiation and no other therapy other than intralesional bleomycin was given. She lived, tumor free, with only a small scar, for 5 years post treatment. Cases 1 and 4 are alive and doing well 3 and 2 years respectively post bleomycin therapy.
In summary, we recommend that stage I Merkel cell carcinoma be treated with bleomycin following the following protocol:
- MCC should be surgically excised.
- If there is adequate renal function, five IU of bleomycin should be injected at the biopsy site once a week for three weeks. Bleomycin is excreted by the kidneys and some older patients may attain high blood levels if kidney function is inadequate.
- Post-treatment follow-up biopsy to verify the MCC has been cured. Patients require long-term follow-up to ensure the early identification of recurrence or metastatic disease.
It is tempting to suggest systemic bleomycin as a chemotherapeutic agent for metastatic MCC, but we have no experience with this to date.
References
1. Toker C. Trabecular carcinoma of the skin. Arch Dermatol 1972; 105: 107-110.2. Agelli M and Clegg L. Epidemiology of primary Merkel cell carcinoma in the United States. J Am Acad Dermatol 2003; 49: 832-841.
3. Bichakjian C, Lowe L, Lao C, Sandler H, Bradford C, Johnson T, and Wong S. Merkel cell carcinoma: Critical review with guidelines for multidisciplinary management. Cancer 2007; 110: 1-12.
4. Feng H, Shuda M, Chang Y, and Moore PS. Clonal integration of a polyoma virus in human merkel cell carcinoma. Science 2008; 319: 1096-1100.
5. Engels E, Frisch M, Goedert J, Biggar R, and Miller R. Merkel cell carcinoma and HIV infection. Lancet 2002; 359: 497-498.
6. Penn I and First MR. Merkel's cell carcinoma in organ recipients: report of 41 cases. Transplantation 1999; 68: 1717-1721.
7. Heath M , Jaimes N, Lemos B, et al., Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol 2008; 58: 375-381.
8. Pectasides D, Pactasides M, and Economopoulos T. Merkel cell cancer of the skin. Annals of Oncology 2006; 17: 1489-1495.
9. McKee P, Calonje E, Granter SR, Pathology of the Skin with Clinical Correlations, 2005, 3rd edition, Vol. 2, Elsevier Limited, pg 1237.
10.Gu J, Polak JM, Tapia FJ, Marangos PJ, and Pearse AG, Neuron-specific enolase in the Merkel cells of mammalian skin. The use of specific antibody as a simple and reliable histologic marker, Am J Pathol, 1981:104; 63-68.
11.Ball NJ, and Tanhuanco-Kho G, Merkel cell carcinoma frequently shows features of basal cell carcinoma: a study of 30 cases, J Cutan Pathol, 2007;34(8):612-619
12. Gupta S, Wang LC, Penas PF, Gellenthin M, Lee SJ, Nghiem P, Sentinel lymph node biopsy for evaluation and treatment or patients with Merkel cell carcinoma. Arch Dermatol 2006; 142: 685-690.
13. Lewis KG, Weinstock MA, Weaver AL, Otley CC et al. Adjuvant local irradiation for Merkel cell carcinoma. Arch Dermatol 2006; 142: 693-700
14. Mortier L, Mirabel X, Fournier c, Piette F, Lartigan E, Radiotherapy alone for primary Merkel cell carcinoma. Arch Dermatol 2003; 139: 1587-1590.
15. Totsuk A, Muller WEG, and Zahn RK, Bleomycin: Action on Growth of Oncogenic RNA Viruses and on Cell Transformation, Arch Virol 2005;48(2):169-179
16. Rakic B, Brulotte M, Rouleau Y, Belanger S, Pezacki JP. Bleomycin is a potent small molecule inhibitor of hepatitis C virus replication. ChemBioChem 2006; 7: 1330-1333.
17. Van ABS and Marx JJM, Use of bleomycin against viral infections, European patent application number EP199990952071, 03/14/01
18. Templeton SF, Solomon AR, and Swerlick RA. Intradermal bleomycin injections into normal human skin. A histopathologic and immunopathologic study. Arch Dermatol 1994; 130(5): 577-583.
19. Gyurova MS, Stancheva MZ, Arnaudova MN, and Yankova RK. Intralesional bleomycin as alternative therapy in the treatment of multiple basal cell carcinomas. Dermatology Online Journal 2006; 12(3): 25.
© 2008 Dermatology Online Journal