Bilobed flap for reconstruction of defects of the helical rim and posterior ear
Published Web Location
https://doi.org/10.5070/D314b5327pMain Content
Bilobed flap for reconstruction of defects of the helical rim and posterior ear
Irene J Vergilis-Kalner MD1,2, Leonard H Goldberg MD1,2,3
Dermatology Online Journal 16 (10): 9
1. Derm Surgery Associates, Houston, Texas. ivergilis@hotmail.com2. Departments of Dermatology, Weill Cornell Medical College, Methodist Hospital, Houston, Texas
3. The University of Texas Medical School, Houston, Texas
Abstract
When contemplating the repair of defects involving the ear, second intention healing and full or split thickness skin grafts are often considered for reconstructive choices. Closing the combined full thickness helical rim and posterior ear defects, however, represents a reconstructive challenge because of the lack of available freely mobile skin anteriorly, superiorly, and inferiorly to the defect. The choice of the bilobed flap circumvents this challenge by rotating the skin and recruiting the tissue from the post-auricular sulcus, the lower pole of the posterior ear, and, if necessary, from the superior area of the neck adjacent to the posterior ear. This bilobed flap also enables an inconspicuous closure of the donor site and provides sufficient blood supply to ensure flap viability in a simple one-stage repair. Herein, we describe two cases in which we used the bilobed flap to rotate skin from the post-auricular surface to reconstruct full thickness skin defects involving the helical rim and posterior ear, with excellent cosmetic results.
Introduction
Defects involving both the helical rim and posterior ear represent a unique reconstructive challenge. The rim of the ear is curved, whereas the skin on the anterior ear is closely adherent to the cartilage and cannot be moved to cover the defect once the dermis is removed. There is little subcutaneous tissue to protect the underlying cartilage, exposure of which may lead to chondritis and pain [1, 2]. Removal of cartilage may cause the ear to become smaller. Furthermore, if the reconstructed helical rim is not smooth, this may result in notching.
Reconstructive possibilities for defects in this location include second intention healing, full or split thickness skin grafts, and primary linear closure, if the defects are small and predominately on the posterior surface of the ear [1]. Away from the helical rim, donor skin from the posterior surface of the ear is easily obtainable and the defect can be closed with a vertically oriented side-to-side closure. Other reconstruction options for the posterior ear, adjacent to and on the helical rim, include the helical rim advancement flap, helical advancement flap, wedge excision, or a post-auricular interpolation flap from the scalp [2]. Many of the local options involve extensive undermining, often into the hair-bearing portions of the scalp [3]. The bilobed flap is a useful technique for transferring local tissue while simultaneously minimizing donor-site deformity [3, 4]. Herein, we describe two cases in which a bilobed flap was used to rotate skin from the post-auricular surface to reconstruct full thickness skin defects involving the helical rim and posterior ear, with excellent cosmetic results.
Description of the procedure
 |  |
| Figure 1a | Figure 1b |
|---|---|
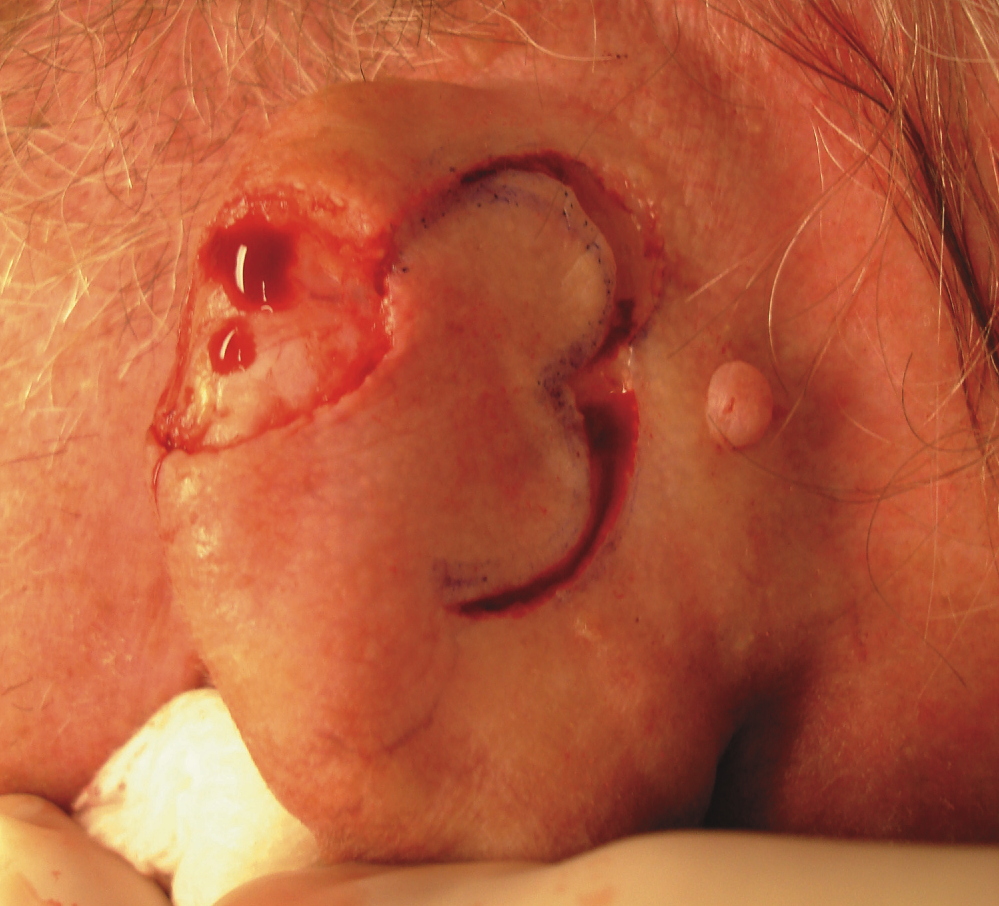
| Figures 1a and 1b. Posterior ear defect involving helical rim; bilobed flap is drawn | |
The tumor is excised and margin control is assured. The resulting defect is assessed to determine reconstruction options. A bilobed flap is drawn adjacent to the defect with the lobes at 90º angles to each other (Figures 1a and 1b). A solution of 0.5 percent lidocaine with epinephrine (1:200,000) is used as tumescent anesthesia for the surrounding skin. The tissue is undermined above the perichondrium. This plane is avascular and does not disturb the blood supply of the flap. Wide undermining of the surrounding skin to get secondary skin movement over the cartilage is possible without nerve and vessel damage because there are no major nerves or vessels in this plane on the posterior surface of the ear.
 |  |
| Figure 2a | Figure 2b |
|---|---|
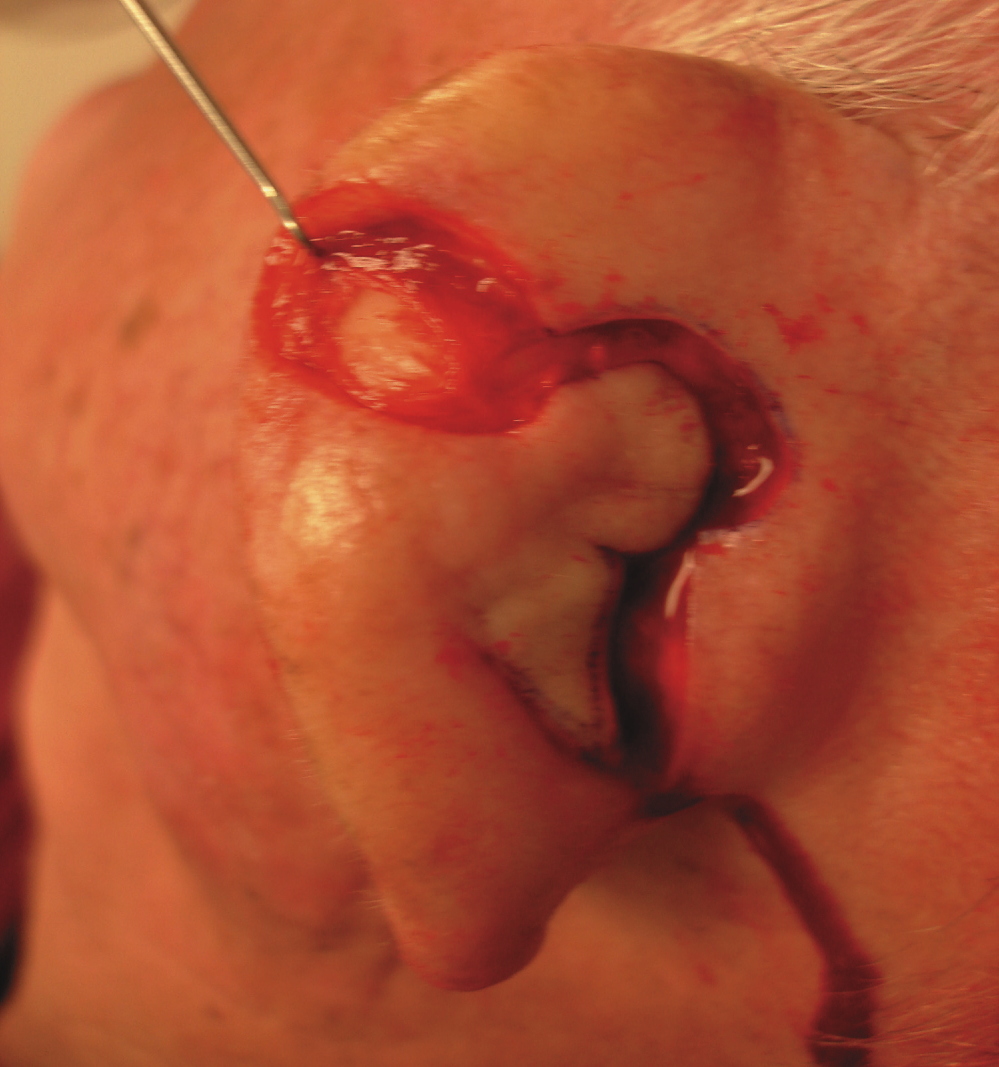
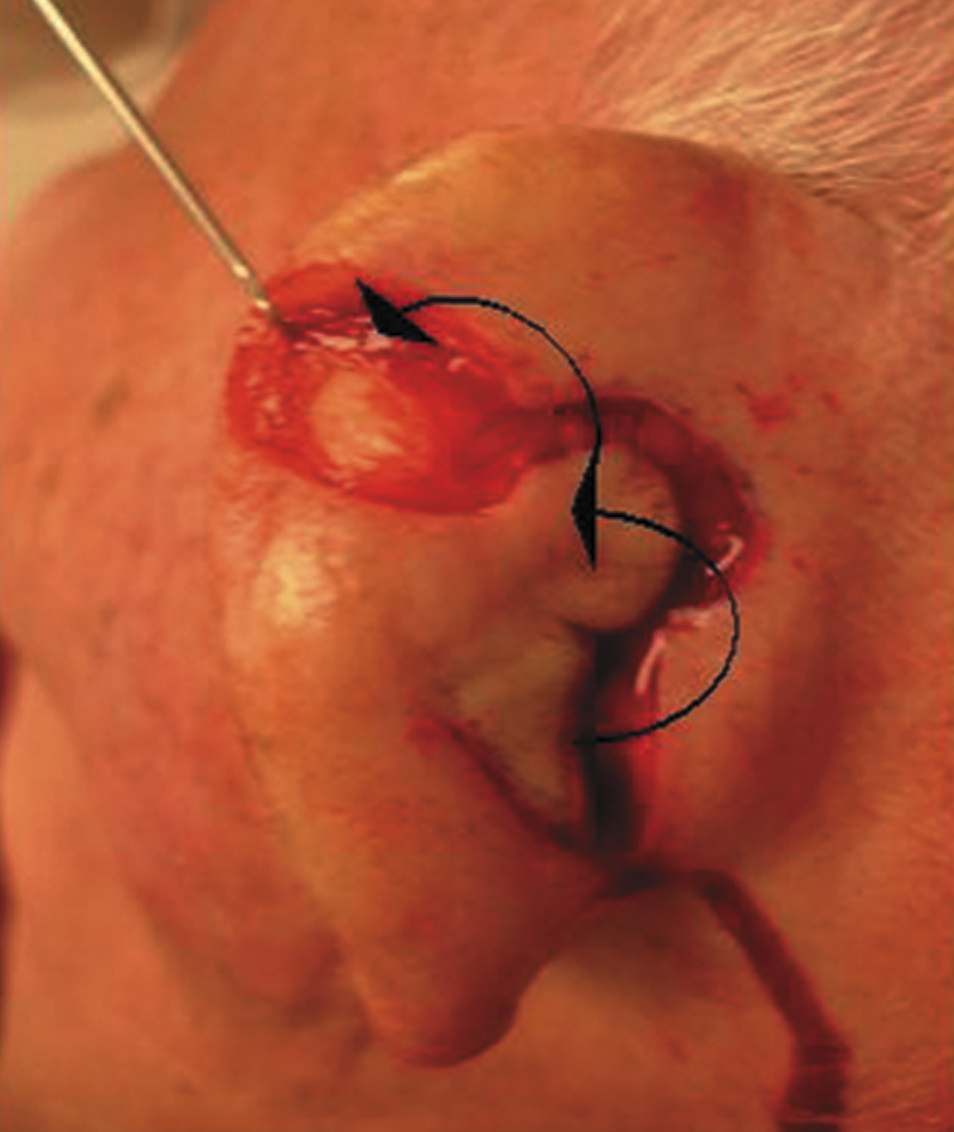
| Figures 2a, 2b, and 2c. Design and outline of the bilobed flap | |
 |
| Figure 2c |
|---|
Once the entire bilobed flap and skin surrounding the defect is adequately mobilized (Figures 2a, 2b, and 2c), the flap is elevated and the primary and secondary lobes are transposed into their respective defects (Figures 3a and 3b).
 |  |
| Figure 3a | Figure 3b |
|---|---|
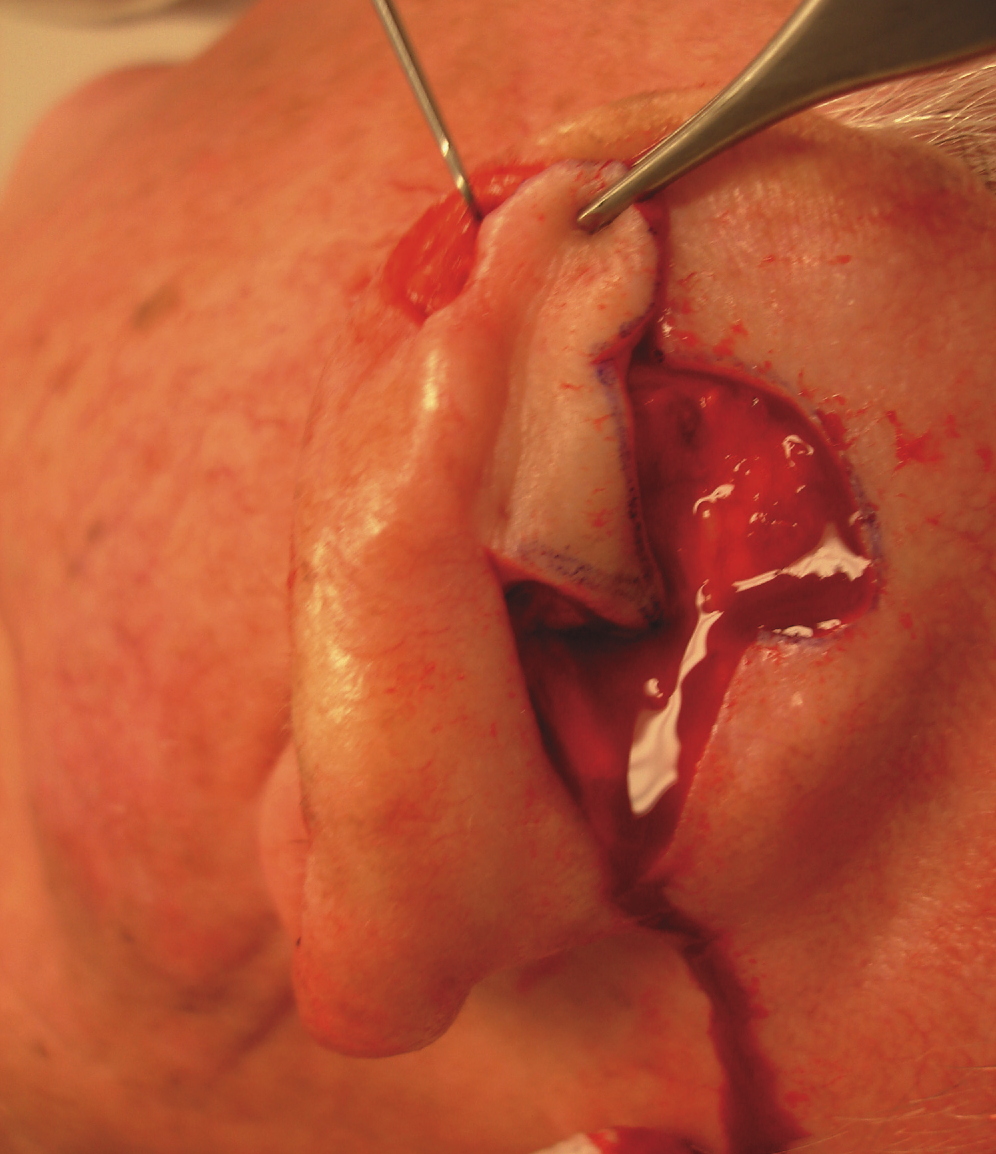
| Figures 3a and 3b. Depiction of primary and secondary lobes transposed into their respective defects. | |
Interrupted 4-0 non-absorbable sutures are placed to establish the ideal flap placement. The primary lobe is used to cover the original defect. The second lobe is then used to cover the secondary defect from the donor site of the primary lobe. Post-auricular advancement is used to close the tertiary defect resulting from this bilobed flap. The epidermis is approximated with a running 5-0 non-absorbable suture with careful attention paid to eversion of wound edges to produce a smooth epidermal surface.
 |  |
| Figure 4a | Figure 4b |
|---|---|
| Figures 4a and 4b. Bilobed flap after being sutured in place. | |
A pressure bandage is applied and left in place for two days. After this time, traditional daily wound care is followed. Figures 4a and 4b demonstrate the flap in place without distortion of the anatomy and good color and texture matching. Figures 5a and 5b show the cosmetic result at the 4-month follow-up.
 |  |
| Figure 5a | Figure 5b |
|---|---|
| Figure 5a and 5b. 4-month follow-up of bilobed flap: anterior and posterior views. | |
Discussion
The helical rim and posterior surface of the ear in men is a common site of occurrence of skin malignancies because of sun exposure [3]. The contour of the ear is determined by the shape of the cartilage. Defects that cause even small changes in the cartilage may alter the shape of the ear and can cause noticeable deformity. Therefore, the surgeon should strive to leave cartilage in place both during the tumor removal, as well as during the subsequent reconstruction.
Techniques used to repair posterior ear defects include simple linear closures, skin grafts if the perichondrium and soft tissue are intact, local rotation flaps, two-lobed advancement flaps from the post-auricular sulcus, and post-auricular interpolation flaps for larger defects of the ear rim [3]. Closing the combined helical rim and posterior ear defects, however, still represents a reconstructive challenge because of the lack of available freely mobile skin anteriorly, superiorly, and inferiorly to the defect. The choice of the bilobed flap circumvents this challenge by using skin from the posterior surface of the ear and, as necessary, from the post-auricular groove. This flap is a one-stage repair in which donor tissue is transferred from the area of excess, such as from the post-auricular sulcus, lower pole of the posterior ear, or superior neck adjacent to the posterior ear, rotated anteriorly, folded forward, and fitted into the defect over the exposed cartilage. There is usually enough skin in the postauricular groove to advance and primarily close the secondary defect created by the rotation of the flap. Consequently, this bilobed flap enables recruitment of tissue from a well-concealed area and can be used to reconstruct a moderate-sized defect on the rim of the ear and on adjacent posterior ear without changing the size of the ear or distorting the contour. This flap also provides coverage to the cartilage that results in a good skin color and texture match.
In 1918, Esser described the use of the bilobed flap, a random pattern flap for reconstruction of nasal tip defects [6]. Esser’s original design required that the angle of tissue transfer be 90º between each lobe of the flap for a total pivotal movement of 180º [6]. This design maximizes the distance that the skin can be moved. However, the wide angles between the two lobes (90º) also maximize the standing cutaneous deformities and the likelihood of creating “trap door” deformities of both the first and second lobes [7]. An advantage of the bilobed flap is that most of the incisions necessary to create the flap produce scars that can be placed parallel to relaxed skin tension lines [7]. Moreover, the second lobe of the transposition flap reduces the overall wound closure tension and provides additional skin to the proximity of the reconstruction [7].
The degree of pivotal movement could be varied from the original 90º between each lobe [7]. In 1989, Zitelli published his experience using the bilobed flap for nasal reconstruction, in which he used a narrow 45º angle of transfer between each lobe, so that the total pivotal movement of tissue occurs over no more than 90º to 100º instead of the classic 180º design [3, 7, 8]. This allowed surgeons to minimize the donor-site deformity by strategically placing the flap donor sites into areas of skin laxity and/or lines of skin tension, thus eliminating the need to excise standing cone deformities [3, 7]. Zimany and others expanded the use of the flap to reconstruct defects on the trunk and soles, although most authors now share the opinion that this flap is most useful for reconstruction of the nose [7, 9].
In our experience, the bilobed flap on the ear has produced good results in the reconstruction of defects post-Mohs micrographic surgery with exposed cartilage on the posterior ear and on or adjacent to the helical rim. In the design of the proposed bilobed rotation flap, the lobes are at 90° from each other, which is essentially the Esser technique. The primary disadvantage of this technique is that it leads to a large dogear that cannot be excised, evident in Figure 4b. However, the site can still heal with a good cosmetic outcome, as demonstrated in Figure 5a.
It is the rotation of the donor tissue that differentiates this flap from the two-lobed advancement flap, previously described by Alam and Goldberg in 2003 [5]. In the two-lobed advancement flap, there is a linear movement of the skin from the post-auricular sulcus to repair posterior ear defects. We find this flap particularly useful for repair of smaller defects on the more posterior aspects of the ear. On the other hand, in the bilobed flap, there is rotation of the tissue with recruitment of the donor tissue from the postauricular sulcus, as well as from the lower pole of the posterior ear and the superior area of the neck adjacent to the posterior ear. It is this rotation and recruitment of the donor tissue from the lower pole of the posterior ear and superior area of the neck, in addition to postauricular sulcus, that differentiates this bilobed flap from the medially based bilobed flap reported by Ricks and Cook in 2005 [10]. We find that our proposed flap is particularly useful to cover moderate- to large-size defects involving both helical rim and its adjacent posterior surface of the ear given the large reservoir of excess donor tissue available to be recruited and rotated to cover the defect. Moreover, this bilobed rotation flap could essentially be used anywhere on the helical rim and adjacent posterior surface of the ear by simply changing the direction of rotation of the donor tissue.
As demonstrated by our two cases, the bilobed flap is a one-stage reconstruction that enables the closure of posterior ear surface defects of varying sizes, extending to or adjacent to the helical rim. This flap utilizes relatively loose postauricular skin, as well as skin from the postauricular groove, or from the superior area of the neck. It allows excellent color and texture match and avoids distorting the architecture of the ear. Furthermore, it enables inconspicuous closure of the donor site and provides sufficient blood supply to ensure flap viability in a simple one-stage repair. Thus, we would like to introduce this bilobed flap for highly aesthetic repair of otherwise difficult to close helical rim and posterior ear defects.
References
1. Goldberg LH, Mauldin DV, Humphreys TR. The postauricular cutaneous advancement flap for repairing ear rim defects. Dermatol Surg 1996, 22: 28-31. [PubMed]2. Justiniano H and Eisen DB. Pearls for perfecting the mastoid interpolation flap. Dermatology Online Journal 2009, 15(6): 2. [PubMed]
3. Cordeiro CN, McCarthy CM, Mastorakos DP, Cordeiro PG. Repair of postauricular defects using cervical donor skin: a novel use of the bilobed flap. Ann Plast Surg 2007, 59: 451-2. [PubMed]
4. Ono I, Yamashita T, Takada T, et al. Reconstruction method with a newly-designed bilobedd flap after excision of tumours of the skin. Scand J Plast Reconstr Surg Hand Surg 2006, 40: 32-40. [PubMed]
5. Alam M and Goldberg LH. Two-lobed advancement flap for cutaneous helical rim defects. Dermatol Surg 2003; 29: 1044-1049. [PubMed]
6. Esser JFS. Gestielte locale Nasenplastik mit Zweizipfligem lappen Deckung des Sekundaren Detektes vom ersen Zipfel durch den zweiten. Dtsch Z Chirurgie 1918, 143: 385.
7. Baker SR: Facial Flaps. St Louis, Mosby, 2002, pgs: 189-211.
8. Zitelli JA. The bilobed flap for nasal reconstruction. Arch Dermatol 1989, 125: 952. [PubMed]
9. Zimany A. The bilobed flap. Plast Reconstr Surg 1953, 11: 424.
10. Ricks M and Cook J. Extranasal applications of the bilobed flap. Dermatol Surg 2005, 31: 941-8. [PubMed]
© 2010 Dermatology Online Journal