Graham-Little-Piccardi-Lassueur syndrome
Published Web Location
https://doi.org/10.5070/D312s800rxMain Content
Graham-Little-Piccardi-Lassueur syndrome
Neelam Vashi MD, Tracey Newlove MD, Julie Chu MD, Rishi Patel MD, Jennifer Stein MD PhD
Dermatology Online Journal 17 (10): 30
Department of Dermatology, New York University, New York, New York Abstract
Graham-Little-Piccardi-Lassueur syndrome (GLPLS) traditionally describes patients with a triad of a multifocal cicatricial alopecia of the scalp, noncicatricial alopecia of the axillae and groin, and a lichenoid follicular eruption. The entity has caused much controversy with respect to both etiology and clinical definition. We present a patient with lichen planopilaris, lichen planus pigmentosus, and nonscarring alopecia of the genitals, who is reminiscent of GLPLS. Recent work shows evidence for autoimmunity in GLPLS. Further elucidation of underlying mechanisms can improve categorization and treatment options in this rare and controversial syndrome.
History
A 42-year-old Asian woman presented to the Charles C. Harris Skin and Cancer Pavilion in September, 2010, for the initial evaluation of asymptomatic, dark lesions of her neck, which had been present for two years. She also had circular areas of pubic hair loss, progressive recession of the frontal hairline, and the loss of eyebrows and eyelashes for six years. She had tried no treatments. Past medical history included hyperthyroidism, which was treated with propylthiouracil. She was taking no medications and reported an allergy to sulfonamides.
Physical examination
 |  |
| Figure 1 | Figure 2 |
|---|
The frontoparietal hairline had perifollicular, keratotic spines and smooth, shiny patches that were devoid of follicular ostia. There was thinning of the eyebrows and eyelashes and ill-defined, reticulated, grey patches on the cheeks, forehead, and neck. There were circular areas of hair loss with preserved follicular ostia on the mons pubis and suprapubic areas.
Laboratory data
A complete blood count, comprehensive metabolic panel thyroglobulin antibody, thyroid peroxidase antibody, urinalysis, C3, C4, and antinuclear antibodies were normal or absent.
Histopathology
 |
| Figure 3 |
|---|
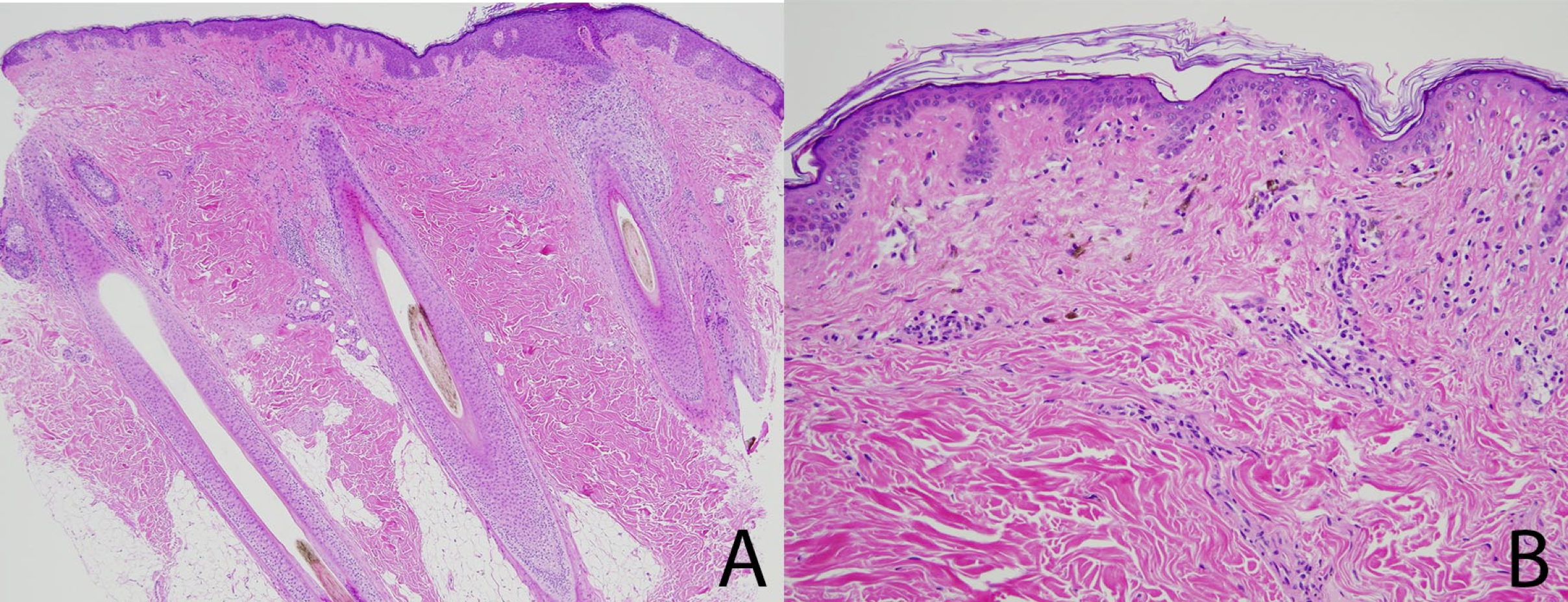
A biopsy specimen from the scalp shows a perinfundibular infiltrate predominantly of lymphocytes that are associated with perifollicular fibrosis, vacuolar alteration, and necrotic keratinocytes (Figure 3A). A biopsy specimen from neck shows vacuolar alteration at the dermoepidermal junction with occasional necrotic keratinocytes and numerous melanophages within the dermis (Figure 3B). A biopsy specimen from the pubic area (not pictured) shows non-scarring alopecia.
Discussion
Graham-Little-Piccardi-Lassueur syndrome (GLPLS) is defined as the triad of multifocal cicatricial alopecia of the scalp, noncicatricial alopecia of the axillae and groin, and a lichenoid follicular eruption.
In 1913, Piccardi described a case of scalp cicatricial alopecia, noncicatricial alopecia in the axillae and groin, and follicular lichen planus. In 1915, Graham-Little published a similar case of a 55-year-old woman, who was referred by Lassueur of Lausanne, Switzerland [1]. To this constellation of findings the name GLPLS was then given [2, 4].
We describe a patient with a triad of lesions reminiscent of GLPLS, which is a rare disorder that usually is described in middle-aged women and that often is associated with severe pruritus [5]. Our patient presented with noncicatricial alopecia of the groin, lichen planopilaris, and lichen planus pigmentosus. Lichen planus pigmentosus, which is an uncommon variant of lichen planus that is characterized by hyperpigmented, brown macules in sun-exposed areas and flexural folds, is not commonly associated with GLPLS [6].
Since its first description in 1913, GLPLS has caused much controversy. In 1953, Silver et al grouped patients with lichen planopilaris, lichen planus, lichen planus acuminatus et atrophicans or lichen spinulosus, and folliculitis decalvans of GLPLS as having the same condition [7, 8]. Clinical, histopathologic, and immunofluorescence findings of these entities also have shown similarities and most investigators consider them to all be types of lichen planus [8, 9].
Many investigators, therefore, consider the simpler classification of GLPLS as a form of follicular lichen planus that is characterized by a lichenoid dermatosis and progressive cicatricial alopecia [1]. The etiology is unknown; however, there are reports linking it to the hepatitis B vaccination, associating it with HLA-DR1 genetic predisposition, and relating it to the complete androgen insensitivity syndrome [3, 10, 11]. Most recently, Rodriguez-Bayona et al proposed an autoimmune link in GLPLS. They described the first autoantibody directed to INCENP protein in humans, which is now considered to be a major autoantigen in GLPLS [12]. INCENP is a component of the centromere during several phases of the mitotic cell cycle and plays a role in chromosome segregation and the regulation of mitosis [12, 13, 14].
The lichenoid dermatosis and scarring alopecia of GLPLS are difficult to treat. Topical, intralesional, and systemic glucocorticoids can provide some relief but are often unsuccessful. Other treatment options include retinoids, phototherapy, cyclosporine, and thalidomide, but the results are variable [5, 15, 16]. Stabilization and improvement of the disease in our patient was attempted with hydroxychloroquine, doxycycline, and tacrolimus ointment. The patient did not respond to tacrolimus ointment. She showed no improvement but was stabilized with a combination of hydroxychloroquine and doxycycline.
References
1. Ghislain PD, et al. Lassueur-Graham Little-Piccardi syndrome: a 20-year follow-up. Dermatology 2003; 206:391 [PubMed]2. Pages F, et al. Syndrome de Lassueur-Graham Little. Ann Dermatol Syphiligr 1961; 88:272 [PubMed]
3. Viglizzo, et al. Familial Lassueur-Graham-Little-Piccardi syndrome. Dermatology 2004; 208:142 [PubMed]
4. de Graciansky P, Pons A. Syndrome de Graham Little-Lassueur. Bull Soc Fr Dermatol Syphiligr 1969; 76:849 [PubMed]
5. Kubba R, Rook A. Graham Little syndrome: follicular keratosis with cicatricial alopecia. Br J Dermatol 1975; 93(Suppl 11):53
6. Pittelkow M, Daoud M. Lichen Planus. In: Wolff K, et al., eds. Fitzpatrick's Dermatology in General Medicine. 7th edition, New York: McGraw-Hill, 2007; 247
7. Silver H, et al. Follicular lichen planus (lichen planopilaris). Arch Dermatol Syphilol 1953; 67:346 [PubMed]
8. Zegarska B, et al. Graham-Little syndrome. Acta Dermatoven APA 2010; 19:39 [PubMed]
9. Wanicowa A. Prypadek zespolu Grahama-Little. Przegl Dermatol 1970; 57:535 [PubMed]
10. Bardazzi F, et al. Graham Little-Piccardi-Lassueur syndrome following HBV vaccination. Acta Derm Venereol 1999; 79:93 [PubMed]
11. Vega Gutierrez J, et al. Graham Little-Piccardi-Lassueur syndrome associated with androgen insensitivity syndrome (testicular feminization). J Eur Acad Dermatol Venereol 2004; 18:463 [PubMed]
12. Rodriguez-Bayona B, et al. Autoantibodies against the chromosomal passenger protein INCENP found in a patient with Graham-Little-Piccardi-Lassueur syndrome. J Autoimmune Dis 2007; 4:1 [PubMed]
13. Towbin H, et al. Electrophoretic transfer of proteins from polyacrylamide gels to nitrocellulose sheets: procedure and some applications. Proc Natl Acad Sci (USA) 1979; 76:4350 [PubMed]
14. Adams, et al. Chromosomal passengers and the (aurora) ABCs of mitosis. Trends Cell Biol 2001; 11:49 [PubMed]
15. George SJ, Hsu S. Lichen planopilaris treated with thalidomide. J Am Acad Dermatol 2001; 45:965 [PubMed]
16. Abbas O. Frontal fibrosing alopecia presenting with components of Piccardi-Lassueur-Graham-Little syndrome. J Am Acad Dermatol 2007; 57(2 Suppl):S15 [PubMed]
© 2011 Dermatology Online Journal