Subungal abcesses secondary to paclitaxel
Published Web Location
https://doi.org/10.5070/D30sm5p3j1Main Content
Subungal abcesses secondary to paclitaxel
M Pilar Albares MD, Isabel Belinchón MD, Jose Carlos Pascual MD, Gloria Vergara MD, Mar Blanes MD, and Isabel Betlloch MD
Dermaatology Online Journal 9(3): 16
From the Department of Dermatology, Hospital General de Alicante, Alicante, Spain. pityalte@hotmail.comAbstract
Various cutaneous side effects, including nail changes, have been associated with taxane chemotherapeutic agents, but usually docetaxel has been implicated. We report a patient with acute paronychia due to paclitaxel administered for treatment of breast cancer.
Docetaxel and paclitaxel are taxoid-antineoplastic agents. These agents are used in the treatment of breast, lung, and ovary cancer.[1] Cutaneous side effects have been associated with treatment with both drugs. Immediate hypersensitivity reaction, erythrodysaesthesis, erythema of the extremities, and macular and erythematous plaques have been reported with docetaxel.[1] Nail changes due to treatment with the taxanes, mainly docetaxel, are reported in 30-40 percent of patients.[2] Hyperpigmentation, Beau's lines, subungal hemorrhage, orange discoloration, onycholysis, and subungal hyperkeratosis have been described with doxetacel treatment.[3] Paclitaxel is not commonly associated with dermatological reactions, although localized skin reactions and tissue necrosis following extravasation have been reported. Less than 2 percent of patients develop nail changes, noted as pigmentation or discoloration of the nailbed.[2] We describe a patient with acute paronychia during her treatment with paclitaxel for breast cancer.
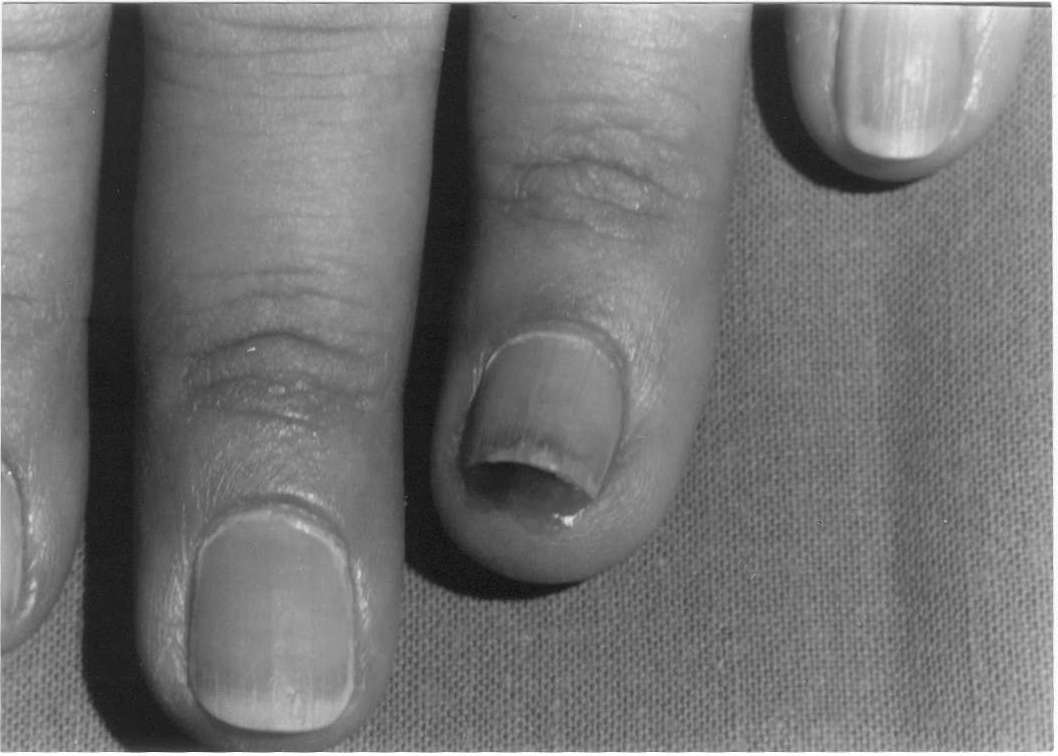 |
| Figure 1 |
|---|
A 37-year-old woman who was undergoing treatment with paclitaxel for poorly-differentiated, infiltrating ductal carcinoma of both breasts was referred to our clinic complaining of nail changes. She noted pain in the fingernails that began two months after she was started on paclitaxel. On examination she had acute paronychia and onycholysis involving all 10 fingers (Fig. 1). Pressure on the nailplate resulted in expression of purulent, serous fluid. Microbiological cultures revealed the presence of Pseudomonas aerouginosa and Candida albicans. Antifungal therapy with fluconazole was prescribed. Paclitaxel was discontinued because of tumor progression. We visited the patient three months later and nail changes had resolved.
Acute paronychia is not a frequent finding with antineoplasic drugs, but it has been decribed with high-dose methotrexate.[4] We have found literature reports of 2 cases of acute paronychia that appeared during the treatment with docetaxel.[1, 3] Recently 4 cases of nailbed purpura followed by pus formation and onycholysis have been reported with paclitaxel.[2] Acute paronychia could possibly result from antineoplastic-agent-induced immunosuppression allowing bacterial or fungal infection. However, considering the fact that all 10 fingers were affected and the similarity of our case to those described in the literature, we believe that paclitaxel is the likely cause of the nail changes in our patient. Direct toxicity to the nailbed or inhibition of angiogenesis have been sugested as possible mechanisms for this reaction.[2]
References
1. Vanhooteghem O, Richert B, Vindevoghel et al. Subungal abscess: a new ungal side-effect related to decetaxel therapy. Br J Dermatol 2000; 143: 445-473.2. Flory SM, Solimando DA, Webster GF et al. Onycholysis associated with weekly administration of paclitaxel. Ann Pharmacother, 1999; 33: 584-586.
3. Correia O, Azevedo C, Pinto-Ferreira E et al. Nail changes secondary to docetaxel(Taxotere). Dermatology 1999; 198: 288-290.
4. Wantzin GL, Thomsen K. Acute paronychia after high-dose methrotexate therapy. Arch Dermatol 1983; 119: 623-624.
© 2003 Dermatology Online Journal