Polypoid dermatofibroma with a slim pedicle: A case report
Published Web Location
https://doi.org/10.5070/D30g5926dvMain Content
Letter: Polypoid dermatofibroma with a slim pedicle: A case report
Hiromichi Kai MD PhD, Hideki Fujita MD PhD, Mizuho Yamamoto MD, Akihiko Asahina MD PhD
Dermatology Online Journal 18 (3): 16
Department of Dermatology, National Hospital Organization Sagamihara National Hospital, Sakuradai, Minamiku, Sagamiharashi,
Kanagawa, JapanAbstract
Dermatofibroma, also called cutaneous fibrous histiocytoma or sclerosing hemangioma, is a fairly common, benign cutaneous tumor. Polypoid dermatofibroma is an unusual and poorly recognized form of this entity. We describe a peculiar case of this variant presenting with a unique morphology characterized by a round flat shape with a slim pedicle, although its histopathological picture was rather typical of that of ordinary dermatofibroma.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|---|
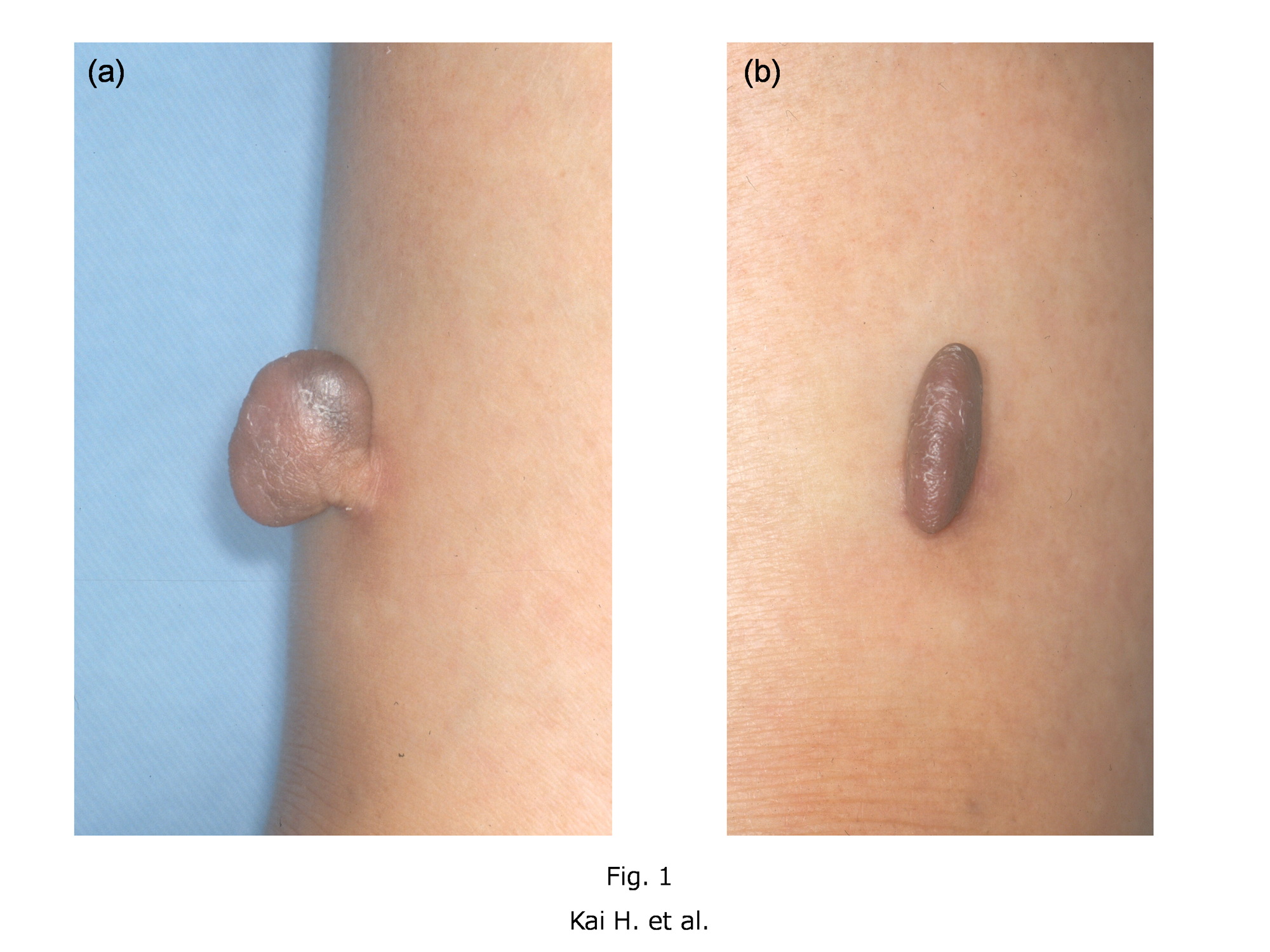
| Figure 1a and 1b. A brown, elastic hard, polypoid nodule of a round flat shape with a slim pedicle, measuring 20 mm x 20 mm
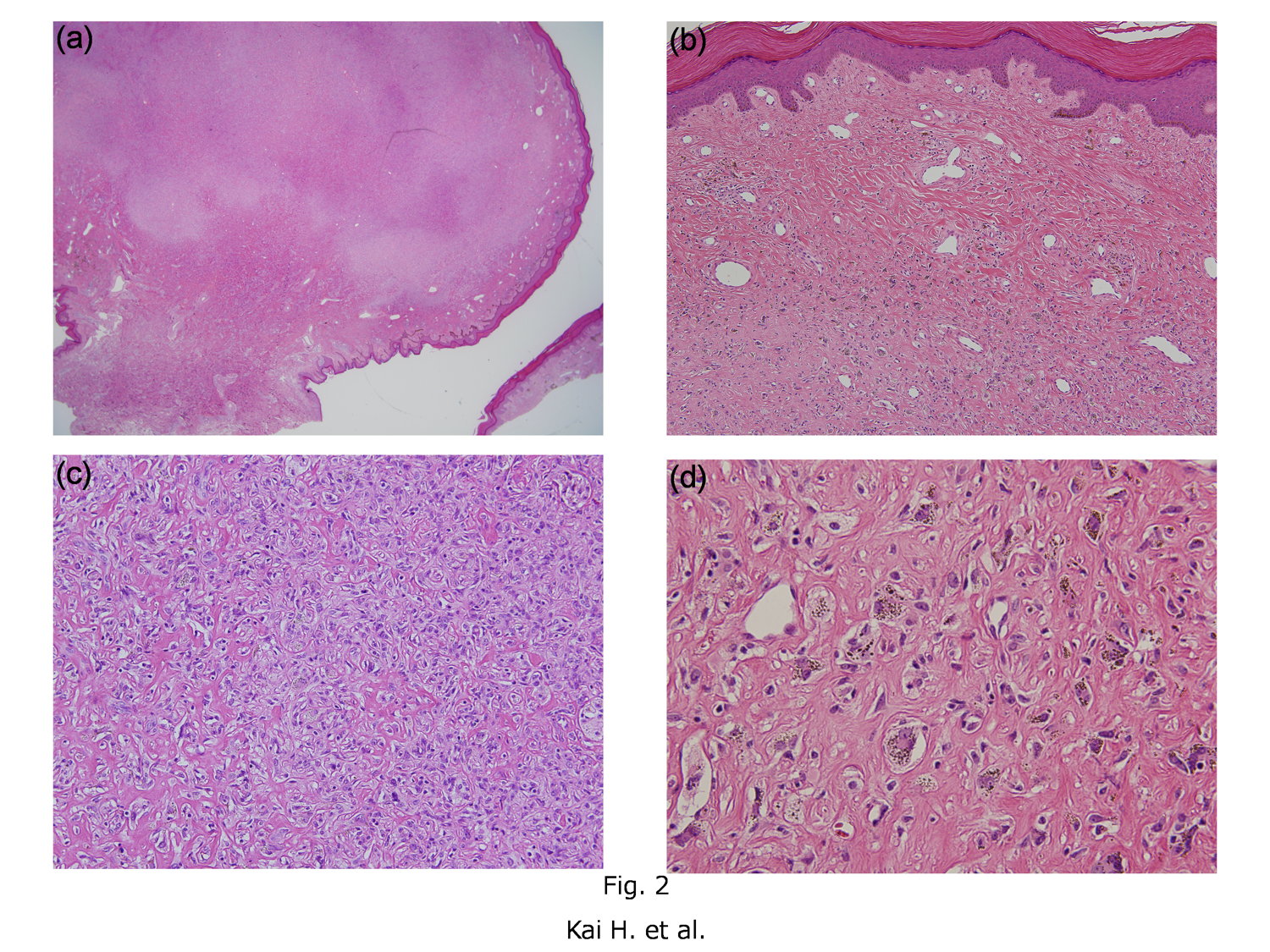
x 5 mm on the extensor side of her right lower leg. Figure 2. (2a) Histopathology of a nodule with aggregation of tumor cells towards the center of the nodule (H&E, x1.25). (2b) The tumor was separated from the overlying hyperplastic and pigmented epidermis by the grenz zone (H&E, x100). (2c) The tumor consisted of interlacing bundles of collagen and rounded epithelioid cells with eosinophilic cytoplasm (H&E, x200). (2d) Histiocyte-like cells and siderophages were observed in some parts of the tumor (H&E, x400). | |
A 68-year-old Japanese woman presented with an asymptomatic polypoid nodule on her leg that had enlarged slowly for the previous 10 years. Physical examination revealed a brown, elastic hard, polypoid nodule of a round flat shape with a slim pedicle, measuring 20 mm x 20 mm x 5 mm on the extensor side of her right lower leg (Figures 1a and 1b). The clinical differential diagnosis included soft fibroma, eccrine poroma, and fibrokeratoma. She had a history of hyperlipidemia, hypertension, and Alzheimer's disease. The polypoid lesion was excised under local anesthesia.
Histopathologically, a low power view of the excised tumor showed aggregation of tumor cells towards the center of the nodule (Figure 2a). The tumor was separated from the overlying hyperplastic and pigmented epidermis (Figure 2b) and consisted of interlacing bundles of collagen and rounded epithelioid cells with eosinophilic cytoplasm (Figure 2c). Histiocyte-like cells and siderophages were also observed in some parts of the tumor (Figure 2d). Characteristically, the pediculate part of the tumor was very slim for the size of the tumor itself and it was composed mostly of hyalinized thick collagen bundles (Figure 2a). The tumor cells did not react with immunohistochemical staining for CD34. Based on these findings, we made the diagnosis of polypoid dermatofibroma with a slim pedicle.
Discussion
Dermatofibroma usually presents as a solitary, slowly growing, firm, indolent, and circumscribed dermal nodule [1]. Although it may occur on any part of the skin, legs are the most frequent sites of occurrence. It is more frequently observed in females than in males and local trauma, such as an insect bite, serves as a precipitating factor [1].
Most cases of dermatofibroma present with a round or ovoid nodule. Polypoid or pedunculated lesions are only rarely observed, comprising only 3 percent of the cases [2]. Of note, two distinct variants of dermatofibroma with unique histopathological features tend to show polypoid lesions. The one is epitheloid fibrous histiocytoma, also known as epithelioid cell histiocytoma [3, 4, 5]. By definition, at least 50 percent of the lesion is composed of rounded or polygonal epithelioid cells with abundant eosinophilic cytoplasm and round to oval nuclei containing small eosinophilic nucleoli. A grenz zone is generally lacking and numerous small blood vessels are a constant feature [6]. Although many epithelioid cells were observed in the tumor, our case was differentiated from epithelioid fibrous histiocytoma by the presence of a well-defined grenz zone and inconspicuous small blood vessels. The other variant of dermatofibroma, called lipidized fibrous histiocytoma, also tends to appear as polypoid [7]. This variant is characterized histopathologically by accumulation of numerous foam cells and stromal wiry hyalinization. In one review, the exophytic appearance was observed in 15 (65%) of 23 tumors, with the polypoid feature in 8 (35%) [7]. In our case, stromal hyalinization was found in the pediculate part of the tumor, but unlike lipidized fibrous histiocytoma, no foam cells were present in the lesion. Based on the histopathological aspect, our case can be described as an “ordinary” type of dermatofibroma rather than the specific variants mentioned above.
In addition to the histopathological picture, the morphological aspect was also quite noticeable in our case. Polypoid dermatofibroma usually has a wide pedicle and shows a smooth elevation above the surrounding skin [8]. Thus, the flat discoid shape with a very slim pedicle, as observed in our case, has not been reported previously. The reason for its unique shape in our case is only speculative. Considering its location, firm underlying tissues, such as tendon or bones, may have prevented its growth deeper in the dermis and led to the polypoid growth [8]. In addition, frequent exposure to mechanical stress may have played a part. This hypothesis is supported by the fact that both epithelioid fibrous histiocytoma and lipidized fibrous histiocytoma occur on the lower extremities in most cases [6, 7]. Finally, it is important to note that dermatofibroma can masquerade as other polypoid tumors and it should be included in the differential diagnosis of polypoid lesions.
References
1. McKee PH, Calonje E, Granter SR. Connective tissue tumors, in Pathology of the skin. McKee PH, Calonje E, Granter SR, editors. 3rd edn. Philadelphia: Elsevier Mosby, 2005; 1742-52.2. Black WC, McGavran MH, Graham P. Nodular subepidermal fibrosis. A clinical pathologic study emphasizing the frequency of clinical misdiagnoses. Arch Surg. 1969 Mar; 98(3):296-300. [PubMed]
3. Jones EW, Cerio R, Smith NP. Epithelioid cell histiocytoma: a new entity. Br J Dermatol. 1989 Feb; 120(2):185-95. [PubMed]
4. Glusac EJ, Barr RJ, Everett MA, Pitha J, Santa Cruz DJ. Epithelioid cell histiocytoma. A report of 10 cases including a new cellular variant. Am J Surg Pathol. 1994 Jun; 18(6):583-90. [PubMed]
5. Singh Gomez C, Calonje E, Fletcher CD. Epithelioid benign fibrous histiocytoma of skin: clinico-pathological analysis of 20 cases of a poorly known variant. Histopathology. 1994 Feb; 24(2):123-9. [PubMed]
6. Luzar B, Calonje E. Cutaneous fibrohistiocytic tumours - an update. Histopathology. 2010 Jan; 56(1):148-65. [PubMed]
7. Iwata J, Fletcher CD. Lipidized fibrous histiocytoma: clinicopathologic analysis of 22 cases. Am J Dermatopathol. 2000 Apr; 22(2):126-34. [PubMed]
8. Sogabe Y, Takahashi A, Tamura A, Ryuzaki K, Ishikawa O. A case of polypoid dermatofibroma. J Dermatol. 2002 Dec; 29(12):786-9. [PubMed]
© 2012 Dermatology Online Journal