Giant cutaneous horn on the lower lip
Published Web Location
https://doi.org/10.5070/D320z279jfMain Content
Giant cutaneous horn on the lower lip
Teresa Pinto-Almeida, Ana Oliveira, Glória da Cunha Velho, Rosário Alves, Mónica Caetano, Manuela Selores
Dermatology Online Journal 17 (12): 10
Department of Dermatology, Centro Hospitalar do Porto – Hospital de Santo António, Porto, PortugalAbstract
Cutaneous horn is a conical hyperkeratotic projection of the skin composed of compact keratin. A wide range of pathologic conditions may be found at its base, including a significant proportion of malignant tumors. A notable, giant cutaneous horn uncovering a keratoacanthoma/well-differentiated squamous cell carcinoma is presented, highlighting the importance of histopathological examination to rule out malignancy because clinical features cannot assure a correct diagnosis.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figures 1 and 2. Giant cutaneous horn on the lower lip | |
A 45 year-old man presented with an asymptomatic exophytic lesion on the lower lip that had grown over the previous year. He was otherwise healthy and was on no regular medication. Physical examination revealed a bifurcate horny yellow projection with a base diameter of 15 mm, which was divided into 2 cones of 30 mm in height each (resembling a bird's beak); the surrounding skin was slightly infiltrated and there was no lymphadenopathy. No other findings were noticed.
 |  |
| Figure 3 | Figure 4 |
|---|---|
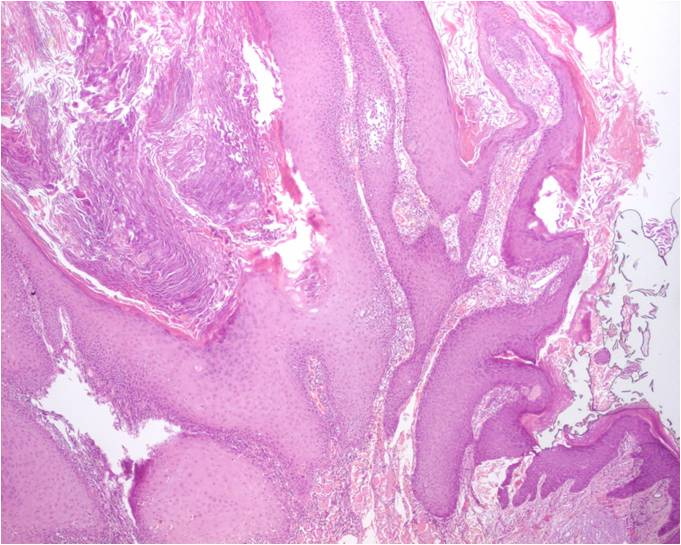
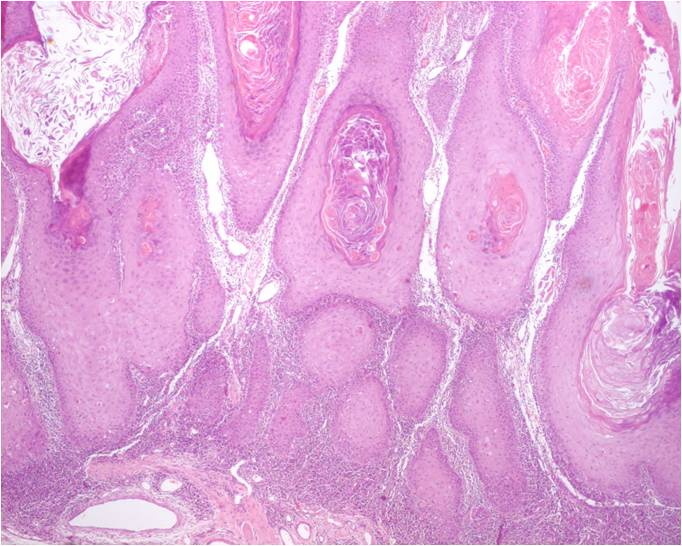
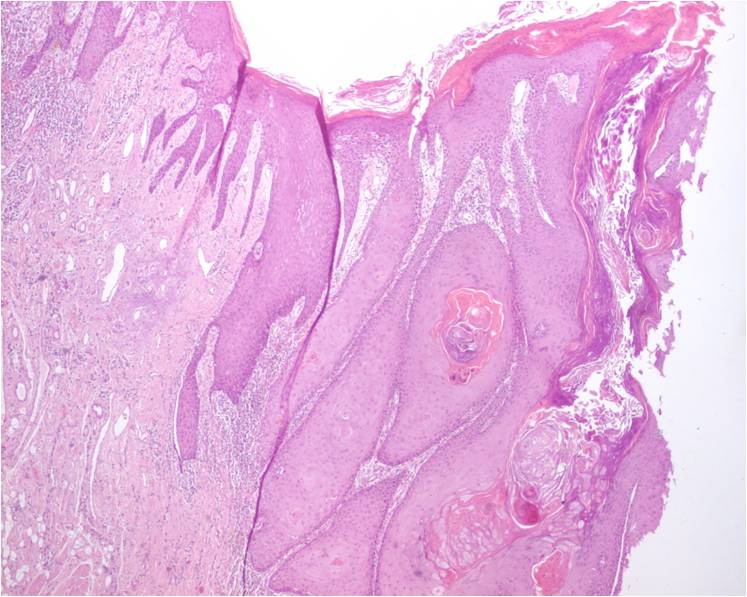
| Figures 3, 4, and 5. Histopathological features of the tumor: epithelial proliferation with exuberant acanthosis, papillomatosis, hyperkeratosis, diskeratosis, and lymphohistiocytic inflammatory at the base. Well-differentiated lip epithelium is seen on the right (Figure 3) and on the left (Figure 5) borders of the lesion. Figure 4. Center of the tumor. (H&E, original magnification x4) | |
 |
| Figure 5 |
|---|
Laboratory workup was unremarkable. Complete surgical excision of the lesion was performed and histopathologic examination showed a symmetrical tumor with a central keratotic core surrounded by an epithelial proliferation with exuberant acantosis, papillomatosis, and hyperkeratosis; diskeratosis and a lymphohistiocytic inflammatory at the base were also evident. The epidermis at both sides of the central core extended over the keratotic area (“lipping”), giving it a crateriform appearance. These features were compatible with either keratoacanthoma (KA) or well-differentiated squamous cell carcinoma (SCC) and the patient was kept under close surveillance. There was no recurrence to date, after 2 years of follow-up.
Discussion
Cutaneous horn is the clinical description of a conical hyperkeratotic projection of the skin composed of compact keratin [1]. It grows in association with many underlying conditions, benign or malignant [1, 2]. Most of them develop on the sun exposed areas and lesions are usually less than 1 cm in high. Giant cutaneous horns are uncommon [3].
Nearly 16 to 20 percent of cutaneous horns have an underlying malignant lesion, most frequently SCC [4, 5]; KA is a less common finding in these circumstances and localization on the lower lip is exceptional [1]. The distinction between KA and well-differentiated SCC cannot always be discerned by histopathologic examination and close clinical follow-up after excision is required, as in our case. Many studies have been carried out with the intent to establish the risk factors and the cutaneous features commonly related to malignancy. The most consistent are: male sex, older age, tenderness at the base of the horn, larger lesions, wide base or low height-to-base ratio, and localization on the nose, pinnae, scalp, back of the hands and forearms. All these features are more likely to be related to a premalignant or malignant histopathological change at the base of the cutaneous horn [3, 4]. Nevertheless, clinical features aren't sufficient to safely establish the malignancy of a cutaneous horn and complete surgical excision and histopathological examination are advised, in order to avoid overlooking more aggressive conditions [6].
Keratoacanthoma is a rapidly growing epithelial tumor with a tendency to spontaneous regression. For some authors, it is considered a variant of SCC because of the potential occurrence of metastases and local tissue destruction [1, 7, 8]. Complete conservative excision is advised in most cases, given the uncertainty regarding the exact behavior of this tumor [1, 7, 8].
References
1. Duncan KO, Geisse JK, Leffell DJ. Epithelial precancerous lesions. In: Fitzpatrick's Dermatology in General 84 Medicine (Wolff K, Goldsmith LA, Katz SI, 83 Gilchrest BA, Paller AS, Leffell DJ, eds), 7th edn. The McGraw Hill Companies, Inc, 2008: 1007-15, 1049-53.2. Gould JW, Brodell RT. Giant cutaneous horn associated with verruca vulgaris. Cutis. 1999;64:111-2. [PubMed]
3. Arvas L, Livaoglu M, Karacal N, Sozen E, Kara B. Giant cutaneous horn with naevus sebaceus. J Plast Reconstruct Aesthetic Surg. 2007;60:1268-9. [PubMed]
4. Yu RCH, Pryce DW, Macfarlane AW, Stewart TW: A histopathological study of 643 cutaneous horns. Br J Dermatol. 1991;124:449-52. [PubMed]
5. Korkut T, Tan NB, Oztan Y. Giant cutaneous horn: a patient report. Ann Plast Surg. 1997;39:654-5. [PubMed]
6. Thappa DM, Garg BR, Thadeus J, Ratnakar C. Cutaneous horn: a brief review and report of a case. J Dermatol. 1997;24:34-7. [PubMed]
7. Karaa A, Khachemoune A. Keratoacanthoma: a tumor in search of a classification. Int J Dermatol. 2007 Jul;46(7):671-8. [PubMed]
8. Cribier B. Keratoacanthoma? Better to say "squamous cell carcinoma, keratoacanthoma type." Ann Dermatol Venereol. 2008 Aug-Sep;135:541-6. [PubMed]
© 2011 Dermatology Online Journal