

We present a new case of a cutaneous bronchogenic cyst on the scapular area in a 2- year-old boy. The asymptomatic nodule over his right scapula had been detected at birth and had been gradually growing. Cutaneous bronchogenic cysts located near the scapula are extremely rare. The proposed mechanism is that the accessory buds from the tracheobronchial tree/primitive foregut migrated from the thorax in an aberrant manner to lie in a periscapular position. Cutaneous bronchogenic cysts are poorly recognized by clinicians because they lack pathognomonic clinical symptoms. The diagnosis is based on the histopathological findings in the majority of cases. Complete excision and histological examination are indicated to confirm the diagnosis, to relieve symptoms, and to prevent complications, such as infection or malignancy.
|
|
| Figure 1 | Figure 2 |
|---|---|
| Figures 1 and 2: Soft, rounded nodule on the scapular area | |
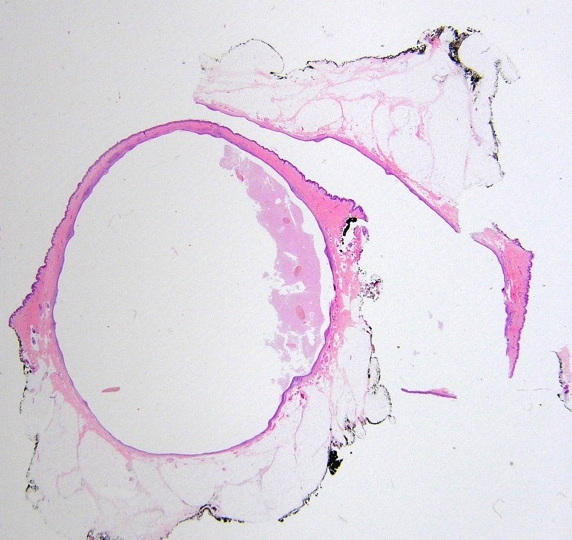
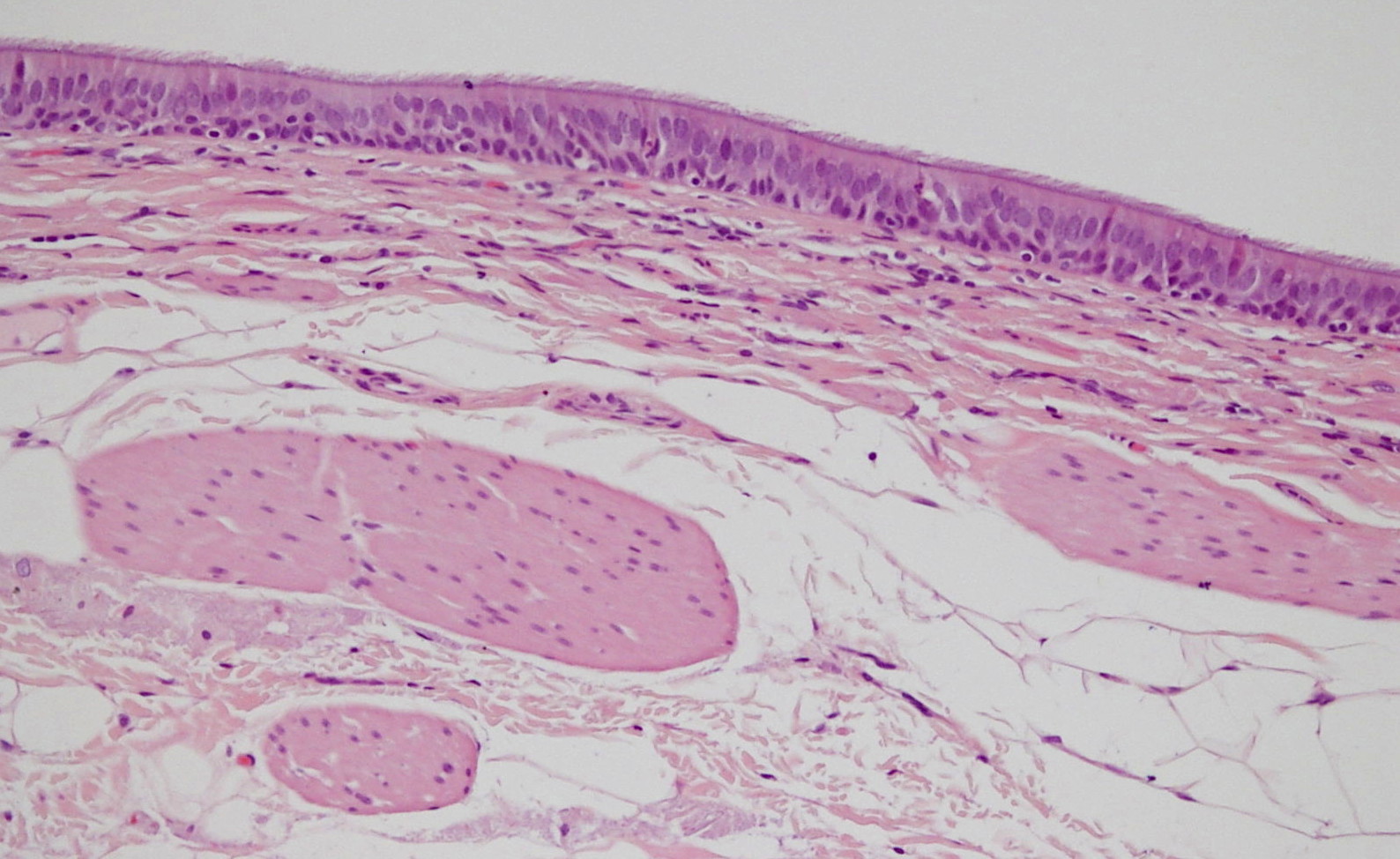
Histopathological study demonstrated a unilocular cyst lined with squamous and pseudostratified ciliated epithelium. Smooth muscle and mucous glands were found in the wall. These features were compatible with cutaneous bronchogenic cyst (Figures 3 and 4). The postoperative course was unremarkable.
 |
 |
| Figure 3 | Figure 4 |
|---|---|
| Figure 3: Skin biopsy specimen showing a unilocular cyst Figure 4. Cyst wall lined by pseudostratified ciliated columnar epithelium. Bundles of smooth muscle are also present in the wall. |
|
Bronchogenic cysts are uncommon developmental anomalies that originate from the primitive tracheobronchial tree. Bronchogenic cysts are rare and prevalence ranges from 1 in 42,000 to 1 in 68,000 [1]. Bronchogenic cysts are commonly located in the lungs or mediastinum.
Cutaneous bronchogenic cysts are even more rare. Seybold and Clagett reported the first case of a cutaneous bronchogenic cyst in 1945. The most frequent location is the suprasternal notch, followed by the presternal area and neck.
Cutaneous bronchogenic cysts located near the scapula are uncommon. In 1971, Fraga et al [2] reported 30 bronchogenic cysts, four of which were located on the scapula or shoulder. To date, about 70 cases of cutaneous bronchogenic cysts have been reported in the literature and only 16 were located in the scapular region [3, 4, 5, 6].
Bronchogenic cyst of the skin is a congenital solitary lesion. Generally it is more prevalent in males than females and appears at birth or shortly after as an asymptomatic mass that increases in size and eventually drains mucoid fluid.
Making the preoperative diagnosis of bronchogenic cyst is very difficult and the diagnosis is histopathological in the majority of cases.
Histologically, bronchogenic cysts are lined by stratified squamous or ciliated, pseudostratified, columnar epithelium. Smooth muscle, seromucous glands, and cartilage may also be present [2].
The main entities in the differential diagnosis include thyroglossal duct cysts and branchial cysts. Thyroglossal duct cysts present as midline cystic nodules on the anterior neck in children or young adults. The characteristic histologic feature is the presence of thyroid follicles composed of cuboidal cells surrounding a homogeneous pink material and a lymphocytic infiltrate.
Branchial cysts appear in the preauricular area, mandibular region, or along the sternocleidomastoid muscle. Histologically, these cysts are lined by stratified squamous epithelium or by pseudostratified ciliated columnar epithelium. They are surrounded by a lymphoid infiltrate that includes lymphoid follicles. Distinguishing branchial from bronchogenic cysts is particularly difficult. Zvulunov et al [7] reported that the presence of lymphoid tissue in cervical branchial cysts and the type of epithelial lining were the most important histologic features for differentiating between cervical branchial cysts and cutaneous bronchogenic cysts.
There are a few reports of cases in which a malignancy has arisen from a congenital bronchogenic cyst in adults. These malignancies included mucoepidermoid carcinoma, malignant pleural mesothelioma, and melanoma [8]. Suen et al reported adenocarcinoma arising from a bronchogenic cyst in an 8-year-old-girl [9].
An explanation for the location of these cysts is difficult. Fraga et al [2] proposed a pattern of migration of tracheobronquial tissue in the course of development.
During embryonic development, the primitive foregut arises in the third week of gestation and divides into the dorsal portion, which elongates to form the esophagus, and the ventral portion, which forms the tracheobronchial tree. Errors in the development of the ventral foregut can give rise to bronchogenic cysts. It is possible that accessory buds from the tracheobronquial tree may migrate to a scapular location. Therefore, the possibility of a congenital bronchogenic cyst should be considered in the event of a cutaneous lesion located in the periscapular area. The definitive treatment is total excision because of the risk of infection and malignant degeneration.
In summary, we present a new case of a cutaneous bronchogenic cyst on the scapular area, which is a rare entity in an unusual location. Frequently, cutaneous bronchogenic cysts are not recognized by clinicians because of the lack of a pathognomonic clinical appearance. Bronchogenic cysts should be included in the differential diagnosis of congenital cystic and nodular lesions. Complete excision and histological examination are indicated to confirm the diagnosis, to relieve symptoms, and to prevent complications, such as infection or malignancy.
© 2012 Dermatology Online Journal