

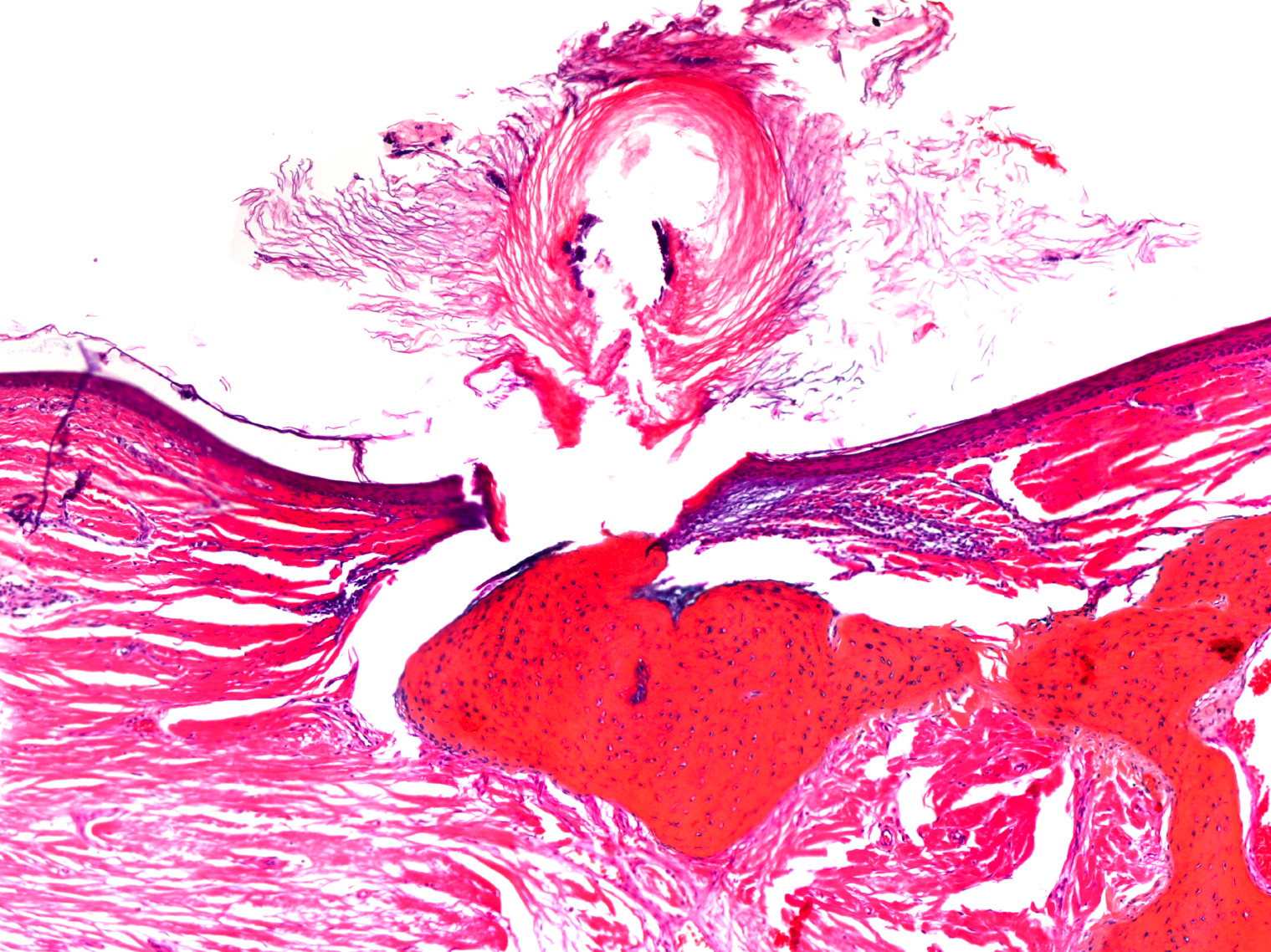
Figure 2. Well-circumscribed nodules of mature lamellar bone surrounded by connective tissue and containing marrow spaces can be observed (H&E, panoramic)
Osteoma cutis, a rare benign condition characterized by the presence of osseous nodules are composed of lamellar bone with osteocytes in the center and osteoclasts in the external area, in the reticular layer of the skin. Osteoma cutis can be either primary, arising de novo in healthy skin, or secondary, developing in association with pre-existing neoplastic or inflammatory skin lesions. We present a 25-year-old man with plaque-like osteoma cutis.
|
|
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Exophytic lesion of the scalp Figure 2. Well-circumscribed nodules of mature lamellar bone surrounded by connective tissue and containing marrow spaces can be observed (H&E, panoramic) |
|
 |
| Figure 3 |
|---|
| Figure 3. Higher magnification reveals transepidermal elimination (H&E, x100) |
A 25-year-old man presented with multiple nodules involving the left forehead. The lesions had been present for 1½ years and had grown progressively. Clinical examination revealed a 2 cm infiltrated and indurated asymptomatic plaque on the forehead (Figure 1). The rest of his cutaneous exam was normal. The patient denied any history of local trauma or acne vulgaris and the previous endocrine evaluation did not show any hormone alterations. Histologic sections are shown in Figures 2 and 3.
Histological sections of skin showed small spicules to large masses of mature bone in the dermis or extending into the subcutaneous tissue. Spicules of bone may enclose areas of mature fat. Because bone located in the superficial dermis causes an irritant reaction, the material may gradually be brought toward the surface and finally eliminated. This is found in islolated primary osteoma cutis with transepidermal elimination. In our patient, the plaque was treated with surgical excision without any evidence of recurrence after 1 year of follow-up.
Osteoma cutis, a rare benign dermatosis is characterized by the presence of osseous nodules in the skin, which are composed of lamellar bone with osteocytes in the center and osteoclasts in the external area, in the reticular layer of the skin. Three theories have been suggested for the pathogenesis of this lesion; 1. Mesenchymal tissue may differentiate into bone in the presence of the tissue injury; 2. Fibroblasts may differentiate into osteoblastic cells; and 3. Displaced pluripotential cells may suffer a metaplastic transformation in the presence of stimulating factors, such as trauma or treatment [1].
Osteoma cutis can be either primary, arising de novo in healthy skin, or secondary, developing in association with pre-existing neoplastic or inflammatory skin lesions (Table 1) [2-10].
Plaque-like osteoma cutis was described by Worret in 1978 and, by definition, is not associated with metabolic alterations, traumatic or inflammatory antecedents, or congenital development through the first year of life) [11].
Some cases of osteoma cutis exhibit the phenomenon of transepidermal elimination [12] similar to granuloma annulare, elastolisis perforans serpiginosa, perforating folliculitis, and perforating pilomatricoma.
Treatment of osteoma cutis generally consists of removal by excision or laser resurfacing. Treatment with the Er:YAG laser may result in less hypopigmentation and scarring than with the carbon dioxide laser. Other reported treatments with unproven efficacy include topical application of tretinoin to provoke transepidermal elimination, oral bisphosphonates,, and the needle microincision-extirpation technique [13, 14].
© 2010 Dermatology Online Journal