

Cutaneous Mastocytosis is not an uncommon condition in the pediatric setting. The eruption can have multiple clinical presentations. We present a case of a 3-month-old child with a solitary mastocytoma who was initially diagnosed with recurrent bullous impetigo. Solitary mastocytoma can present as a blister. Although bullous impetigo is a common diagnosis in children and it would be tempting to make that diagnosis in the presence of a positive skin swab culture, clinicians always have to be mindful of secondary impetiginization of another primary skin disease process.
|
|
| Figure 1 | Figure 2 |
|---|
A 3-month-old infant presents to the pediatric dermatology clinic with a solitary lesion on the left lower leg. At birth the parents noticed a slightly erythematous area. There was no significant past medical history; milestones were normal.
Intermittently this area will form a superficial blister that will cover the majority of the surface area of the lesion; the blister will rapidly rupture to form a scab. At a one point she was diagnosed with a superficial bacterial infection after culturing Moraxella spp. from the area.
The blistering did respond to topical antibiotics, but a well-demarcated 1 cm x 2 cm erythematous plaque remains (Figures 1 and 2).
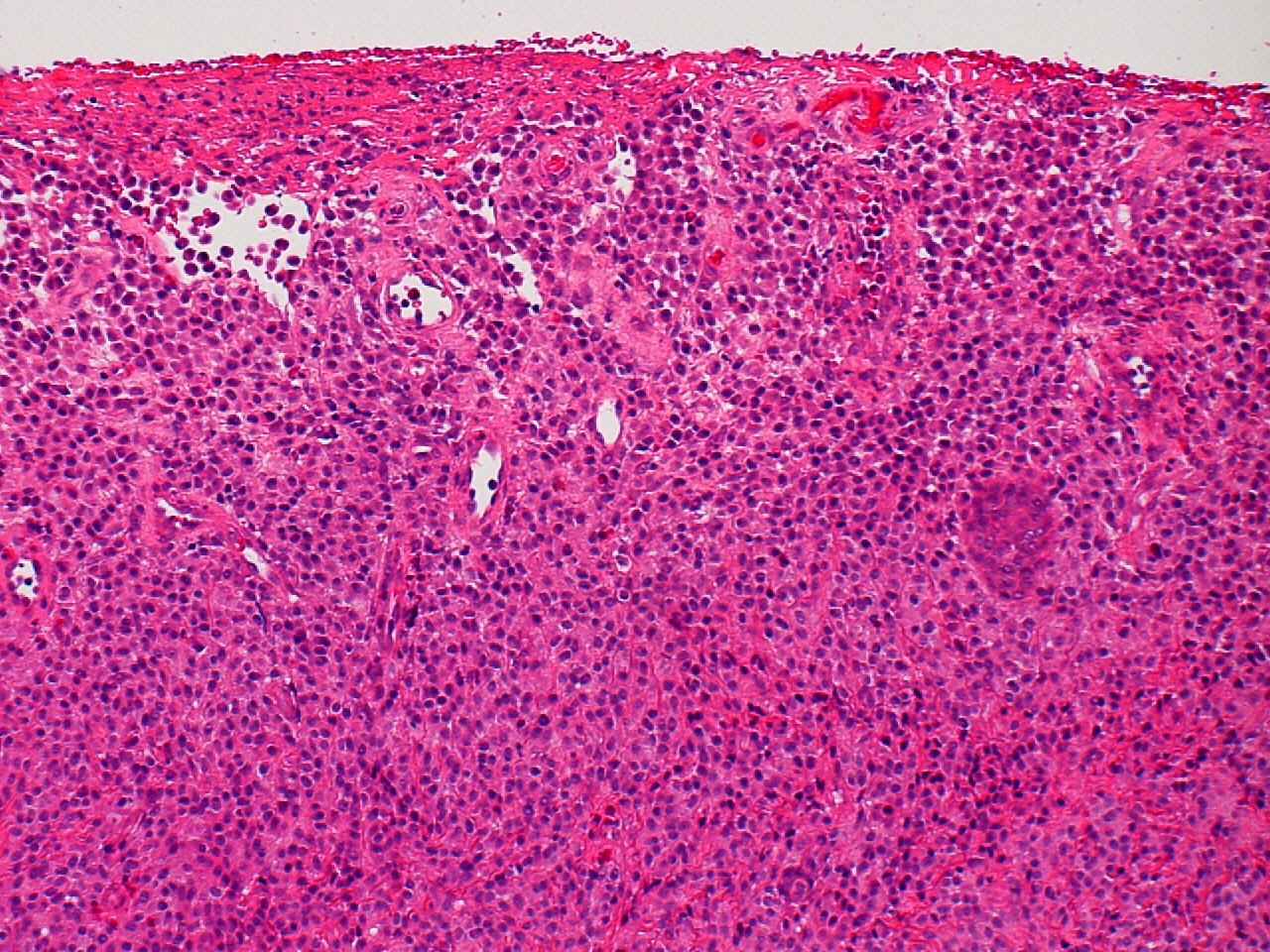
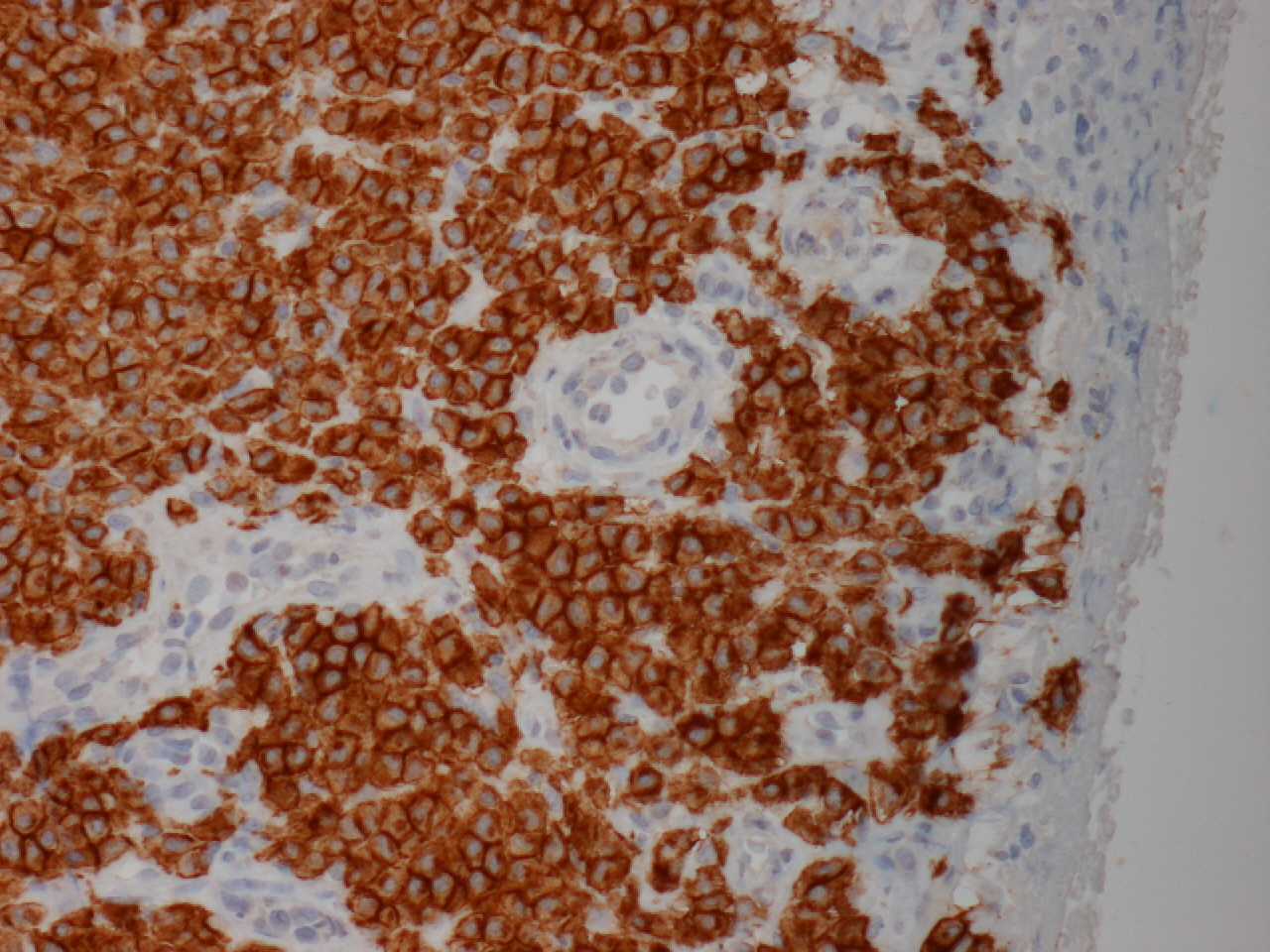
A diagnostic biopsy shows surface ulceration covered with fibrous exudate. The dermis shows sheets of monomorphic cells with oval shaped vesicular nuclei and a moderate to abundant granular cytoplasm. Scattered eosinophils are also present (Figure 3). The cells are strongly positive for CD117 (Figure 4).
 |
 |
| Figure 3 | Figure 4 |
|---|
|
|
| Figure 3 | Figure 4 |
|---|---|
| Figure 3. There is a dense dermal cellular infiltrate with overlying ulceration. The tumor cells have abundant eosinophilic
cytoplasm and uniform darkly staining nuclei. (H&E, x10) Figure 4. Immuohistochemistry for CD117 show strong cytoplasmic positivity. |
|
Mastocytosis is defined as a heterogenous group of disorders with an abnormal accumulation of mast cells (MCs) that can occur anywhere in the body [1].
The course of mastocytosis is varied and depends on the subtype and on the age of onset. In children, mastocytosis is commonly cutaneous mastocytosis (CM) and often transient when compared with that in adults, in whom systemic disease is more prevalent [2].
Little is known about the pathogenesis of mastocytosis and factors contributing to disease progression. Stem cell factor (SCF) is a cytokine that induces the differentiation of MCs from their progenitors, which in turn express a specific tyrosine kinase receptor for SCF (KIT) that is encoded by the KIT proto-oncogene. A “gain of function mutation” in KIT is associated with enhanced survival and autonomous growth of MCs. Such mutations, particularly KIT D816V, are often detected in patients with systemic mastocytosis (SM) [3]. It is not known which factors contribute to the abnormal accumulation and distribution of MCs in the skin in CM, because only a subgroup of patients with CM displays a KIT mutation [3]. Anti-c-kit (CD117) staining has a high specificity and a high sensitivity for MCs in paraffin sections. This staining is against the c-KIT membrane receptor. It stains MCs even after they have degranulated [1].
In 2001 a consensus classification based on the behavior/course of the disease rather than its clinical description was proposed and approved by the World Health Organization. In this consensus classification, mastocytosis is divided into three major groups consisting of cutaneous mastocytosis CM, systemic mastocytosis SM (indolent, aggressive, and with associated clonal hematologic illness of an origin other than the mast cell line), and the extremely rare localized extracutaneous MC neoplasms (not described in children). The WHO classification also includes major and minor criteria to assist in differentiating CM from SM [4].
The WHO classification of CM includes the following categories: maculopapular cutaneous mastocytosis (MPCM) or urticaria pigmentosa (UP), diffuse CM, and solitary mastocytoma of skin [4]. Other authors also recognize a 4th category of telangiectatic cutaneous mastocytosis [1].
In children, mastocytosis is mostly cutaneous, therefore Heide et al. proposed a protocol for the diagnosis and management of CM in children, stating that in most cases bone marrow biopsies and treatment are usually not required [1].
Therapy in isolated CM may be omitted. In cutaneous mastocytosis with complaints of itch, redness, and swelling, avoiding foods, which according to the history provoke the lesions, may be of benefit. Systemic therapy, consisting of a combination of H1- and H2-blockers (and oral sodium cromoglycate) may be helpful [1]. Intralesional injections of steroid have been reported as a useful treatment in solitary mastocytoma, as has the use of 0.05 percent betamethasone dipropionate under occlusion [5]. Surgical excision of a solitary mastocytoma remains a rapid, simple, and effective treatment [6]. Another treatment option for localized CM is the use of topical pimecrolimus [7].
Mastocytomas constitute 10-30 percent of childhood CM. This condition is arbitrarily defined as less than 5 lesions. They present as oval slightly elevated plaques or nodules that are yellow to brown in color with a diameter of 1-5 cm [8].
In one large series of 112 patients, most solitary mastocytomas were either present at birth or developed within the first month of life [9]. Another review of 180 pediatric cases of mastocytosis found that one-third of patients had a mastocytoma, which was present at birth in over 40 percent and appeared during the first year of life in most of the remainder [10].
Flushing, mild tenderness, and formation of bullae may occur with temperature change or trauma or when the lesion is rubbed. However, extracutaneous involvement is uncommon [6].
Vesiculation or frank blistering of lesions occurs commonly in infancy and may be confused with bullous impetigo, epidermolysis bullosa, or cigarette burns [11, 12].
Our patient had a diagnostic biopsy that was consistent with the diagnosis of a solitary mastocytoma. The child was otherwise healthy and showed normal developmental milestones. A full blood count, electrolyte, and kidney and liver function tests were normal.
We treated the lesion with a moderately potent topical steroid (Mometasone Furoate 0.1%) that stopped blistering and flattened the lesion, although it did not completely resolve. We are keeping the patient under regular follow-up and the possibility of excising the lesion completely if spontaneous resolution does not occur at a later stage has been discussed with the parents.
© 2010 Dermatology Online Journal