
A 65-year-old man with stage IV small lymphocytic lymphoma (SLL), diagnosed 7 months prior to presentation, had been on treatment with pentostatin, cyclophosphamide, and rituximab for 4 months. He had an ongoing dermatitis that first developed when he started chemotherapy and has recently developed a pruritic papulo-vesicular eruption on his trunk, especially his lower back. Three weeks before presentation, he developed cellulitis that was treated with IV daptomycin and moxifloxacin. He applied topical triamcinolone cream 0.1 percent to his ongoing dermatitis which resulted in improvement. Two days after completing IV antibiotics, he noted crops of new, very pruritic papules and small vesicles on his back that ruptured, leaving erosions. He also complained of new areas of erythema on his glans penis.
On physical exam there were multiple erythematous papules on the patient's chest and back with predominance on the lower back (Fig. 1). A few clear vesicles and erosions were present. Balanitis was also noted on the glans.
|
| Figure 1 |
|---|
Cultures of the back lesions and the glans penis were negative for bacteria and fungi. Two skin biopsy specimens were obtained from the lesions on the patient's back (Figure 2).
 |
 |
| Figure 2 | Figure 3 |
|---|
Both biopsy specimens revealed a superficial and deep primarily lymphocytic infiltrate with eosinophils and focal areas of epidermal necrosis. Acantholysis compatible with Grover's disease was not identified, but epidermal necrosis complicated the evaluation. Immunohistochemical studies revealed that the infiltrate consisted primarily of CD5-positive T-cells. No cells positive for CD 20, CD79A, or PAX-5 were noted. CD79a and PAX-5 were used to exclude a population of CD5-positive B-cells compatible with SLL since the lymphoid cells of patients treated with rituximab often lose CD20 antigenicity.
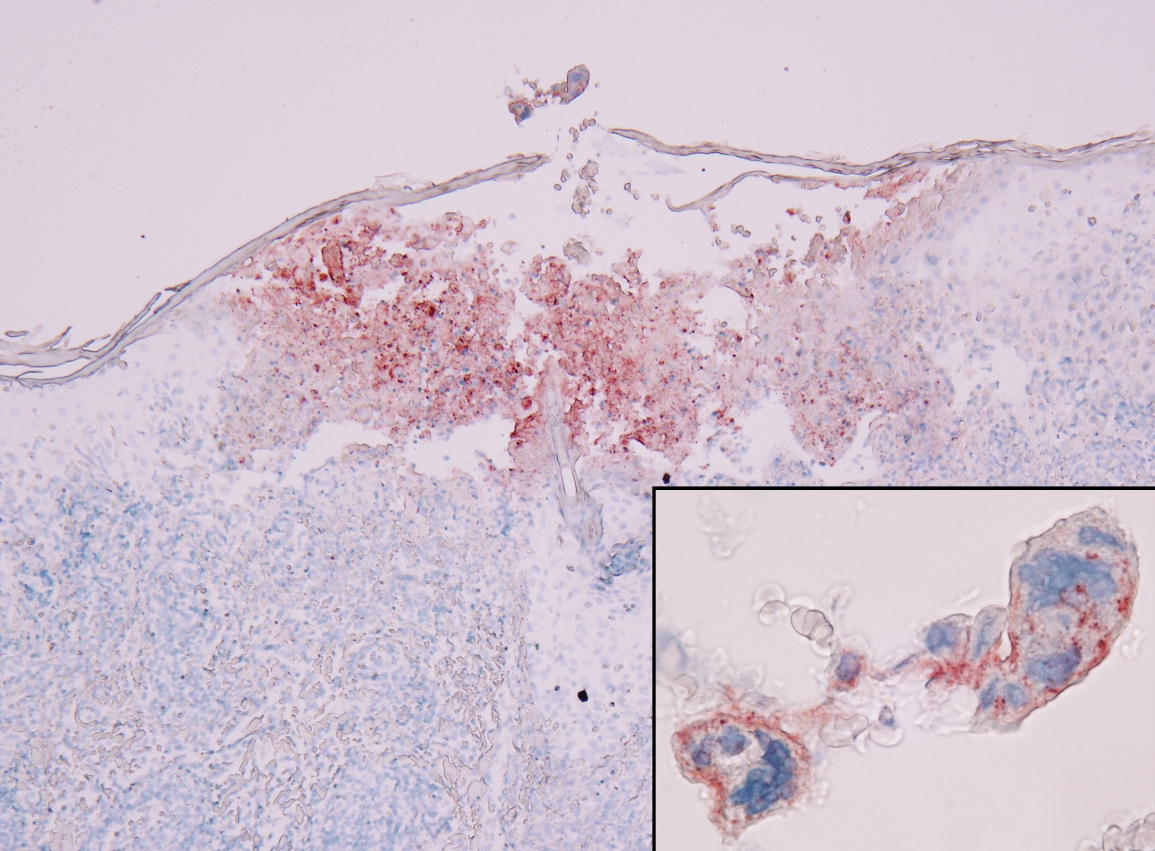
A specific immunohistochemical stain for herpes simplex virus (HSV) I and II reacted with keratinocytes within the erosions (Fig. 3). Multinucleated keratinocytes with nuclear molding were also demonstrated (Inset, Fig. 3). A stain for varicella zoster virus was negative. The patient's trunk lesions and balanitis improved rapidly on oral acyclovir at 800 mg four times daily; however, he continued to have the eosinophilic perivascular and perifollicular lymphocytic infiltrate, consistent with dermatitis.
This patient had chronic eosinophilic dermatitis that began while he was taking highly immunosuppressive therapy for B-cell SLL and then developed papulo-vesicular lesions. Grover's disease which is associated with both immunodeficiency and malignancy, including leukemia and lymphoma[1], was the initial clinical diagnosis.
Surprisingly, keratinocytes in the lesion stained positively for HSV. Kaposi's varicelliform eruption (KVE) or dissemination of cutaneous herpes simplex in adults usually affects patients who have any of many primary dermatologic conditions. Kaposi's varicelliform eruption has been reported following atopic dermatitis (eczema herpeticum), keratosis follicularis (Darier's disease), pemphigus foliaceus, mycosis fungoides, ichthyosis vulgaris, bullous pemphigoid, familial benign pemphigus (Hailey-Hailey disease), burns, skin grafts, staphylococcal scalded skin syndrome, multiple myeloma, erythroderma following steroid withdrawal, aftermath of dermabrasion, and transient acantholytic dermatosis (Grover's disease) [2, 3].
Small lymphocytic lymphoma and its leukemic variant, B-cell chronic lymphocytic leukemia (CLL), are the most common form of lymphoid malignancy in Western countries. The malignant cells are mature B-lymphocytes with a unique surface immunotype (CD5+, CD20+, CD23+) [4]. Advanced CLL/SLL results in immunosuppression secondary to hypocomplementemia, hypogammaglobulinemia, and abnormal T-cell function which may have caused his eosinophilic dermatitis [5]. Increased susceptibility to viral infections, particularly infection with herpes virus, has been reported [6], and these infections can have atypical or severe presentations [7]. The increased susceptibility to HSV infections in CLL/SLL may be due to the fact that the neoplastic B-cells express increased levels of the herpes virus entry protein A (Hve A), which binds to HSV glycoprotein D, mediating viral entry. Although these CLL B-cells are able to effectively present antigen, the cytotoxic T-cell and natural killer response are impaired [8].
Immunosuppression increases the risk of opportunistic infections, including HSV. Iatrogenic immunosuppression affecting both T- and B-cells can be caused by the chemotherapeutic regimen this patient was receiving. Purine analogs such as pentostatin which decreases T-cells [8], alkalating agents such as cyclophosphamide, and monoclonal antibodies targeted to immune cells such as rituximab (targeting CD20+ B-cells)[9] have all been demonstrated to increase a patient's risk to certain infections, including HSV.
This patient's clinical presentation of disseminated cutaneous HSV was atypical and was thought to be Grover's disease initially. Kaposi's varicelliform eruption has been reported following Grover's disease [3], and the pathological appearance of Grover's disease has been reported to have similarities to that of herpes infections [10]. Whitmore et al reported a case of a pruritic papulo-vesicular eruption with multinucleated giant cells and discussed the diagnostic challenge in distinguishing Grover's disease from disseminated herpes. The authors decided that the patient had Grover's disease although immunohistochemical stains for herpes simplex or zoster were not performed.
Our patient with SLL developed an eosinophilic dermatitis after immunosuppressive therapy, followed by a classic presentation of Kaposi's varicelliform eruption. This highlights the importance of considering the possibility of atypical presentations of cutaneous herpes infections in patients who are immunosuppressed or have an underlying hematological malignancy.
© 2007 Dermatology Online Journal