
Eyelid lesions frequently are a diagnostic challenge. We report a case of a 46-year-old woman with a 5-year history of yellowish symmetric progressively growing papules on the eyelids, resembling xanthelasma. A skin biopsy was performed that revealed the rare variant of clear cell syringoma. The lesions were treated with CO2 laser and surgical excision; there was no evidence of recurrence after 6 months of follow-up.
Answer: Clear cell syringoma
|
| Figure 1 |
|---|
| Figure 1. Multiple bilateral symmetrical papules on the eyelids, slightly firm and yellow to tan and ranged from 2 to 6 mm in the long axis |
A 46-year-old woman presented with a 5-year history of bilateral symmetrical papules on the upper and lower eyelids. The papules had progressively grown in number and dimension. Besides cosmetic concerns, the patient noted that the lesions were asymptomatic and she was otherwise healthy.
Physical examination revealed multiple bilateral symmetrical papules on the eyelids, slightly firm and yellow to tan, ranging from 2 to 6 mm in the long axis (Fig. 1). An incisional biopsy specimen was obtained (Figs. 2A & 2B).
 |
 |
| Figure 2A | Figure 2B |
|---|---|
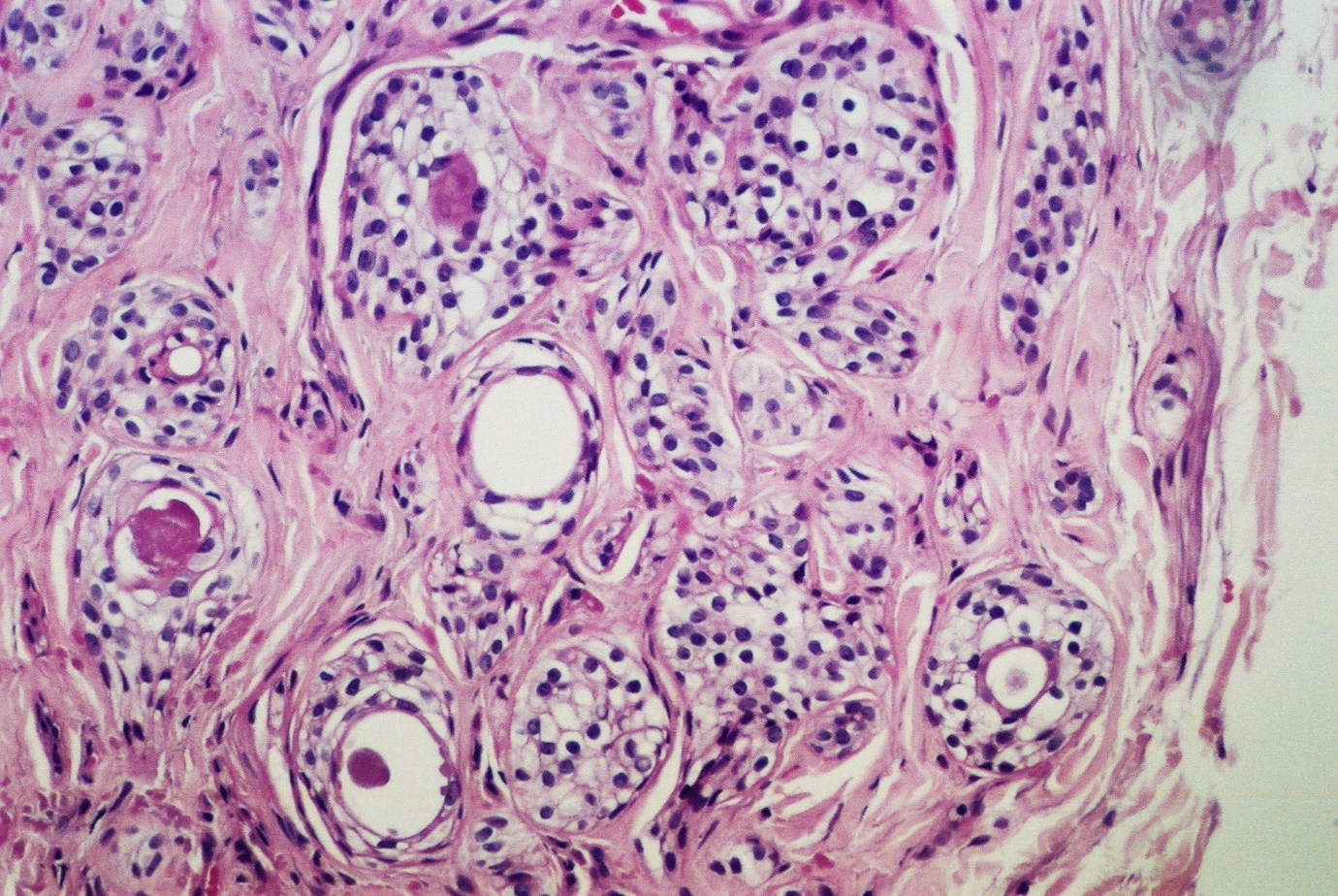
| Figure 2A. Clear cell nests in the upper dermis, surrounded by fibrous stroma and amorphous material in the intraductal space
(H&E, x40) Figure 2B. PAS staining showed reactive spots in the cytoplasm and intraductal space |
|
Histological examination revealed some clear cell nests in the upper dermis, surrounded by fibrous stroma and amorphous material in the intraductal space. Periodic acid-Schiff (PAS) staining showed reactive spots in the cytoplasm and intraductal space.
The smaller lesions were treated with CO2 laser and the larger ones were removed with surgical excision. The cosmetic results were very good and there was no evidence of recurrence after 6 months of follow-up.
Syringoma is a common benign epithelial tumor that derives from eccrine ducts [1, 2]. They are adenomas of the acrosyringium, the intraepidermal portion of the eccrine sweat duct [3]. Clinically, they consist of small, translucent, asymptomatic papules, 2 to 3 mm in size, frequently on the eyelids and the upper cheeks. These tumors develop predominantly in women at puberty or later in life. Microscopically, there is a proliferation of small ducts, usually covered by a double layer of cells surrounded by fibrous stroma; horny material may be present in the ductal space [1].
In 1972, Headington et al. [4], first reported a rare variant type of syringoma, "clear cell glycogenosis in multiple syringoma," in which ductal cells have a clear watery cytoplasm, with glycogen granules stained by PAS. They are clinically indistinguishable from classic syringoma and are more frequently reported in association with diabetes mellitus [3, 5]. That association was not present in this case, as well as in other reports [2]. Furthermore, this case presented with yellowish papules resembling xanthelasma. However, histologically, clear cell syringomas were observed and PAS-positive granules were found in the cytoplasm of the clear cells.
The pathogenesis of clear cell syringoma is still unknown [5]. The frequent onset of syringoma at or around puberty, together with an increased frequency in women and the expression progesterone receptors by many syringomas, strengthens the hypotesis that hormonal influences may be important in their pathogenesis. The reason for glycogen accumulation is unclear, though a deficiency or decreased activity of phosphorylase has been suggested [3].
Some authors consider that clear cell syringoma is a metabolic variant of conventional syringoma because both types show differentiation into the transitional portion between the acrosyringium and the dermal duct [5].
The optimal treatment of syringoma in not fully determined. Some therapeutic options have included laser ablation and surgical excision, with variable results.
© 2009 Dermatology Online Journal