
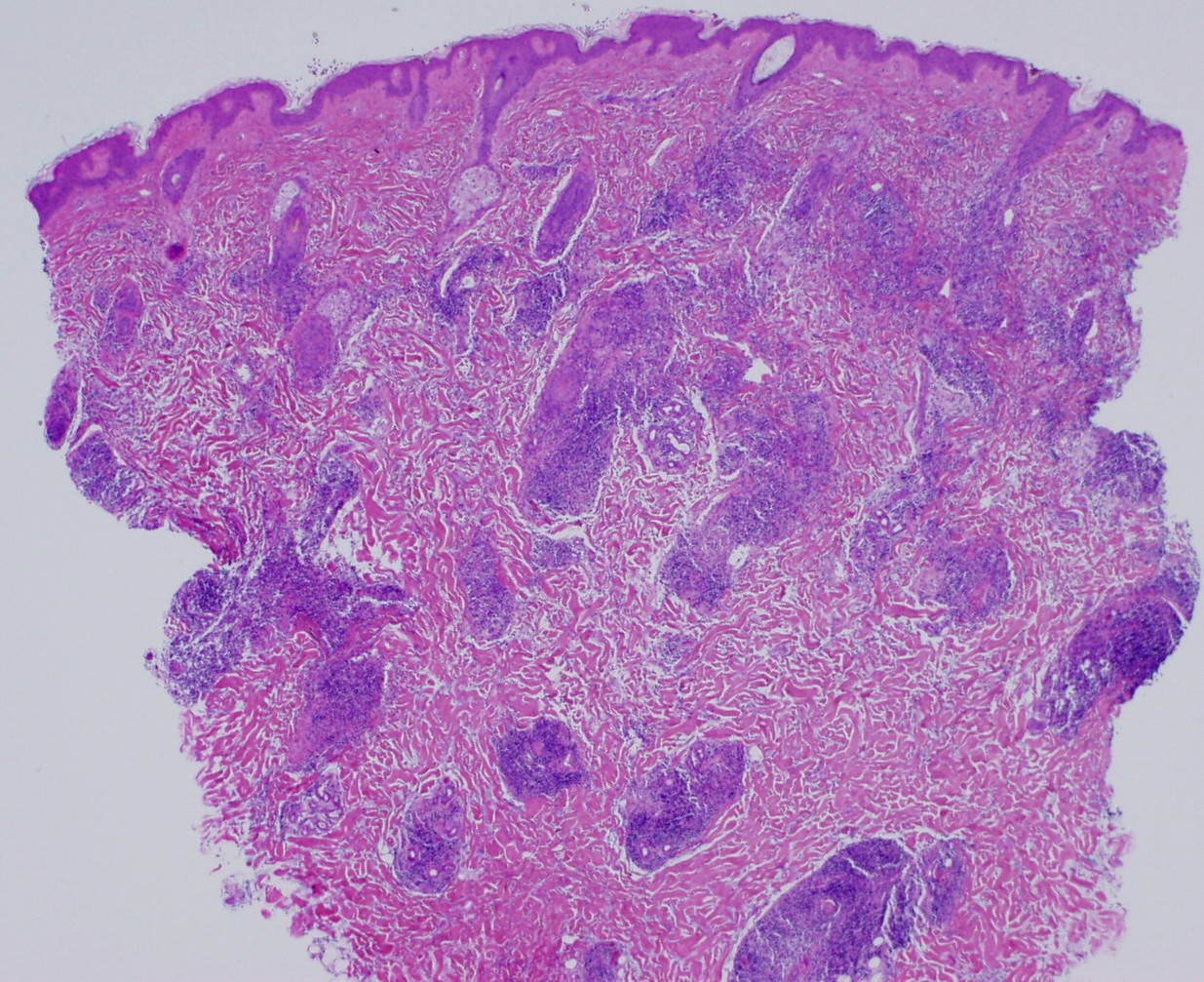
Figure 2. Histologic examination showing a prominent, superficial and deep perivascular and periadnexal predominately lymphocytic infiltrate. Interstitial mucin deposit is present in the dermis. (H&E, x2)
An 18-year-old woman presented with a one-year history of erythematous to slightly violaceous indurated papules and plaques on the face, earlobes, neck, upper arms, chest, and upper back.
|
|
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Left view of the face showing additional lesions present in the earlobe and the posterior auricular region of the
neck. Figure 2. Histologic examination showing a prominent, superficial and deep perivascular and periadnexal predominately lymphocytic infiltrate. Interstitial mucin deposit is present in the dermis. (H&E, x2) |
|
An 18-year-old woman presented with a one-year history of erythematous to slightly violaceous indurated papules and plaques on the face (Figure 1), earlobes, neck, upper arms, chest, and upper back. The lesions did not have scale. The patient reported significant photosensitivity and worsening of lesions after sun exposure, but was otherwise healthy. Serology for antinuclear antibody was negative. Basic laboratory workup including complete blood count, chemistry panel, and urinalysis was normal.
 |
 |
| Figure 3 | Figure 4 |
|---|---|
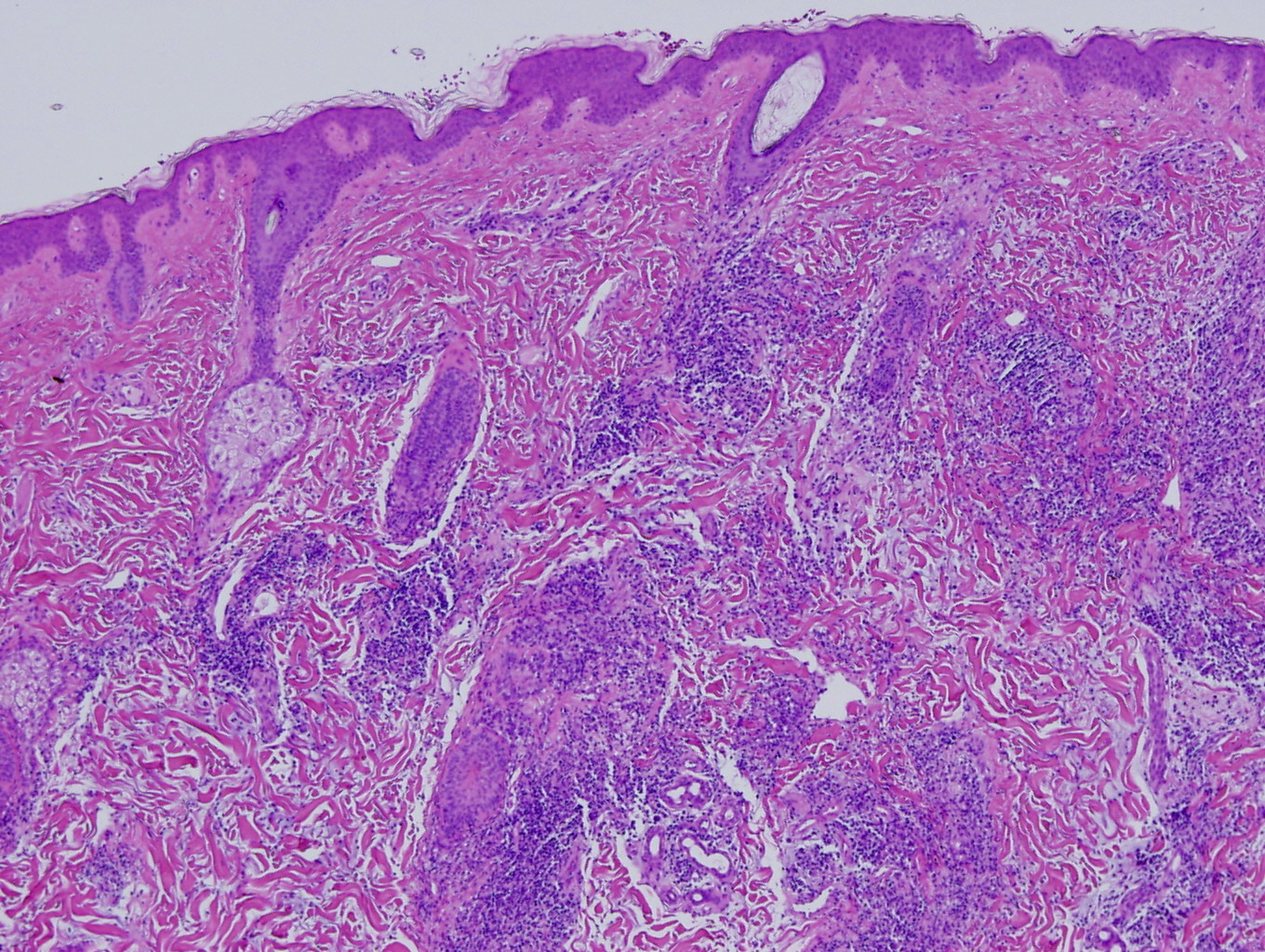
| Figure 3. A view of the epidermis, including the dermal-epidermal junction, showing no significant pathological change (H&E,
x4) Figure 4. A high power view of perivascular and periadnexal predominately lymphocytic infiltrate and intradermal mucin deposits. (H&E, x40) |
|
Punch biopsy specimens from the posterior auricle (Figures 2 through 4) and the upper back were obtained.
The biopsy specimens showed a prominent, superficial, and deep perivascular and periadnexal predominately lymphocytic infiltrate. Interstitial mucin deposit was present in the dermis. The epidermis was essentially unremarkable (Figure 2).
Treatment with hydroxychloroquine 200 mg twice a day and sun protection resulted in a nearly 80 percent improvement of skin lesions without scarring or dyschromia within one month.
Lupus erythematosus (LE) is an autoimmune disorder with a wide spectrum of clinical presentations. Cutaneous LE (CLE) is commonly classified into acute, subacute (SCLE), and chronic CLE (CCLE). Chronic CLE can be further subclassified into discoid LE (DLE), lupus erythematosus tumidus (LET), and several other subtypes, with DLE being the most common subtype [1].
Lupus erythematosus tumidus is a rare form of CCLE that was first described by Erich Hoffman in 1909 and further characterized by Gougerot and Bournier in 1930 [1, 2, 3, 4]. Lupus erythematosus tumidus commonly affects young to older adults with a slight male predilection [2]. Patients with LET usually present with succulent, urticaria-like, non-scarring, reddish or violaceous plaques that occur on sun-exposed skin including face, trunk, and upper extremities. Lesions below the waist have rarely been reported [1, 3]. Intense photosensitivity is one of the major characteristics seen in patients with LET.
Patients with LET are usually negative for antinuclear antibody (ANA) and follow a benign course without systemic manifestations. However, an ANA-positive patient with systemic lupus erythematosus presenting with concurrent LET has also been reported [2]. Clinical presentation of LET closely resembles that of DLE, Jessner lymphocytic infiltrate of the skin, polymorphous light eruption, and reticular erythematous mucinosis (REM). DLE has follicular plugging, which is not present in LET. Some believe that Jessner lymphocytic infiltrate of the skin, REM, and LET are one and the same. Polymorphous light eruption may closely simulate LET, but a biopsy can distinguish the two entities.
Histological analysis of skin lesions is necessary to establish the diagnosis of LET. Moderate to dense, fairly well-circumscribed, superficial and deep lymphocytic dermal infiltrate in a perivascular and periadnexal pattern are the most frequent features.
Interstitial mucin depositions are frequently observed in the reticular dermis. Epidermal changes that are commonly observed in the other forms of CLE, particularly DLE, such as follicular plugging, hyperkeratosis, and vacuolar degeneration of the dermoepidermal junction are minimal or absent [1]. In LET, direct immunofluoresence for immunoglobulin or complement components is usually negative at the dermoepidermal junction or around the papillary and reticular dermal blood vessels. In comparison, up to 60 percent and 90 percent of SCLE and DLE lesions, respectively, are positive for direct immunofluorescence at the dermoepidermal junction [2]. Patients with LET generally have a good response to sun protection and antimalarial treatment; the lesions usually clear without scarring or dyschromia, providing additional valuable clues in differentiating LET from other disorders. Correlation of the clinical, serological, and histological features is necessary to arrive at the correct diagnosis of LET.
The patient’s lesions nearly completely cleared with hydroxychloroquine 200 mg twice daily and her disease remains stable on this regimen one year later.
© 2010 Dermatology Online Journal